
Issuer Free Writing Prospectus dated January 3, 2018
Filed Pursuant to Rule 433
Relating to Preliminary Prospectus Supplement dated January 2, 2018
Registration No. 333-207876
Atara Biotherapeutics, Inc. (the “Company”) has filed a Registration Statement on Form S-3 (including a prospectus and a prospectus supplement) with the Securities and Exchange Commission (the “SEC”) for the offering to which this communication relates. Before you invest, you should read the prospectus and prospectus supplement and other documents the issuer has filed with the SEC and incorporated by reference in the prospectus and the prospectus supplement for more complete information about the issuer and this offering. You may get these documents for free by visiting EDGAR on the SEC website at www.sec.gov. Copies of the preliminary prospectus supplement and the accompanying prospectus related to this offering may be obtained from J.P. Morgan, by mail at J. P. Morgan Securities LLC, c/o Broadridge Financial Solutions, 1155 Long Island Avenue, Edgewood, NY 11717 or by telephone at 866-803-9204; or from Cowen, by mail at Cowen and Company, LLC, c/o Broadridge Financial Services, Attention: Prospectus Department, 1155 Long Island Avenue, Edgewood, NY 11717 or by telephone at 631-274-2806. The final terms of the offering will be disclosed in a final prospectus supplement to be filed with the SEC.
On January 2, 2018 and January 3, 2018, an employee of the Company sent emails to three potential investors that read substantially as follows:
Happy new year [and congrats on your new role]! I’ve thought a lot about our meeting last year as we put together the new ATRA investor presentation attached. You [guys] may have heard that we are marketing an offering today after starting our Phase 3 studies last week. Let us know if you would like to connect with JP Morgan or Cowen to learn more.
I look forward to [catching up soon.][keeping in touch!]
Best regards,
On January 3, 2018, an employee of the Company sent an email to one potential investor that read substantially as follows:
Attached is our new investor presentation. If you’re interesting in the offering today, please let me know and I would be happy to connect you to JP Morgan or Cowen.
Best regards,
On January 3, 2018, after learning of the emails and pursuant to Rule 164(c) of the Securities Act of 1933, as amended, the Company sent the following email to these potential investors:
Dear [potential investor],
My earlier email should have included the following important information:
Atara has filed a registration statement (including the base prospectus) (File No. 333-207876) and a preliminary prospectus supplement with the SEC for the offering to which this communication relates. Before you invest, you should read the base prospectus and the preliminary prospectus supplement and other documents we filed with the SEC for more complete information about Atara and this offering. You may access these documents through the SEC’s website at www.sec.gov. Alternatively, you may obtain a copy of the preliminary prospectus from J.P. Morgan Securities LLC, c/o Broadridge Financial Solutions, 1155 Long Island Avenue, Edgewood, NY 11717, or by telephone at (866) 803-9204 or from Cowen and Company, LLC, c/o Broadridge Financial Services, Attn.: Prospectus Department, 1155 Long Island Avenue, Edgewood, NY, 11717, by calling (631) 274-2806 or by faxing (631) 254-7140.
Sincerely,
January 2018 Nasdaq: ATRA
Disclaimer This presentation and the accompanying oral presentation contain forward-looking statements made pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. All statements other than statements of historical facts contained in this presentation, including statements regarding the completion, timing and size of the proposed public offering, our future results of operations and financial position, business strategy, product candidates, regulatory approvals, the initiation, timing, progress, and results of future preclinical studies and clinical trials and our research and development programs, ability to sell, manufacture or otherwise commercialize our product candidates, research and development costs, timing and likelihood of success, plans and objectives of management for future operations, any royalty payments, and our ability to obtain and maintain intellectual property protection for our product candidates, are forward-looking statements. These statements involve known and unknown risks, uncertainties and other important factors that may cause our actual results, performance or achievements to be materially different from any future results, performance or achievements expressed or implied by the forward-looking statements. These and other important risk factors are described more fully under the heading “RiskFactors” in Atara Biotherapeutics, Inc.‘s (Atara) annual report on Form 10-Q filed with the Securities and Exchange Commission (SEC) on November 9, 2017, including the documents incorporated by reference therein and subsequent filings with the SEC. Because forward-looking statements are inherently subject to risks and uncertainties, some of which cannot be predicted or quantified and some of which are beyond our control, you should not rely on these forward-looking statements as predictions of future events. The events and circumstances reflected in our forward-looking statements may not be achieved or occur and actual results could differ materially from those projected in the forward-looking statements. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained herein, whether as a result of any new information, future events, changed circumstances or otherwise. Certain information contained in this presentation and statements made orally during this presentation relates to or is based on studies, publications, surveys and other data obtained from third-party sources and Atara’s own internal estimates and research. While Atara believes these third-party studies, publications, surveys and other data to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third-party sources. In addition, no independent source has evaluated the reasonableness or accuracy of Atara’s internal estimates or research and no reliance should be made on any information or statements made in this presentation relating to or based on such internal estimates and research. The content of this presentation is subject to copyright, which will be asserted by Atara and no part of this presentation may be reproduced, stored in a retrieval system, or transmitted in any form or by any means without prior permission in writing from Atara. Registration Statement Atara has filed a registration statement (including the base prospectus) (File No. 333-207876) and a preliminary prospectus supplement with the SEC for the offering to which this communication relates. Before you invest, you should read the base prospectus and the preliminary prospectus supplement and other documents we filed with the SEC for more complete information about Atara and this offering. You may access these documents through the SEC’s website at www.sec.gov. Alternatively, you may obtain a copy of the preliminary prospectus from J.P. Morgan Securities LLC, c/o Broadridge Financial Solutions, 1155 Long Island Avenue, Edgewood, NY 11717, or by telephone at (866) 803-9204 or from Cowen and Company, LLC, c/o Broadridge Financial Services, Attn.: Prospectus Department, 1155 Long Island Avenue, Edgewood, NY, 11717, by calling (631) 274-2806 or by faxing (631) 254-7140. This presentation shall not constitute an offer to sell or a solicitation of an offer to buy any securities and shall not constitute an offer, solicitation or sale in any state or jurisdiction in which such an offer, solicitation or sale is not permitted. 2
Offering Summary Issuer Atara Biotherapeutics, Inc. Ticker ATRA Offering Size $100 million (all primary shares); 15% Over allotment option Lock-up 60 days Agreement Continued clinical development of our product candidates, including tabelecleucel, those targeting MS, as well as continued Use of Proceeds pre-commercial preparations for tabelecleucel; and to fund working capital and other general corporate purposes. Book Runners J.P. Morgan; Cowen Expected Pricing Wednesday, January 3rd post-close 3
Building a Leading Off-the-Shelf T-Cell Immunotherapy Company Late-stage Innovative Validated cancer T-cell proprietary off-the-shelf cancer targets –immunotherapy tab-cel™ T-cell immunotherapy growing link of EBV with FDA Breakthrough technology platform pathogenesis in MS and Therapy and EMA autoimmune diseases PRIME designations Transform the lives of patients with serious medical conditions Evidence Safety of efficacy –³50% profile – few treatment Developing response rate in two related serious adverse World-class oncology indications; events T-cell manufacturing Expanded access protocol at over 10 sites Global in U.S. commercial plan Tab-cel™ (tabelecleucel): formerly known as ATA129 4
A Pioneer in Off-the-Shelf T-Cell Immunotherapy –At an Inflection Point ADVANCING INNOVATIVE ROBUST PIPELINE CLEAR TAB-CEL IN TECHNOLOGY EXPANSION STRATEGIC HEMATOLOGIC & PLATFORM OPPORTUNITIES FOCUS SOLID TUMORS ï,— Proprietaryï,— Two Phase 3ï,— Encouraging early ï,— Key milestones off-the-shelf T-cell EBV+PTLD results in expected in next 18 immunotherapy studies initiated progressive months technologies multiple sclerosisï,— Preparing for PTLD ï,— Phase 1/2 NPC ï,— Versatile PD-1 combo studyï,— CMV commercialization therapeutic planned in 2018ï,— Leverage power of ï,— BKV and JCV applications the platform platform NPC: Nasopharyngeal carcinoma; CMV: Cytomegalovirus; BKV: Virus isolated from a renal transplant patient with initials B.K.; JCV: John Cunningham Virus 5
Innovative Proprietary Off-the-Shelf T-Cell Immunotherapy Technology Platform Allogeneic T-Cell Cell Selection Bioengineering Manufacturing Algorithm Two complementary Scalable production Match patients to most technologies processes efficacious T-cell line 1) Broad and 2) Targeted One lot yields therapy Based on over a decade antigen recognition for many patients of clinical experience HLA: human leukocyte antigen 6
Developing Innovative Therapeutic Advantages for Off-the-Shelf T-Cell Immunotherapies Available in No pre- Precision Two hour 3-5 days treatment targeting monitoring with T-cells required with limited off following short delivered from target activity IV infusion inventory 7
Off-the-Shelf T-Cell Technology Platform with Broad Potential Applications Programs Focused in Three Major Therapeutic Areas Autoimmune Viral Oncology Diseases Diseases ï,— Hematologyï,— Multiple sclerosisï,— CMV – EBV+PTLD (MS) ï,— BKV ï,— Solid tumors ï,— Other autoimmune ï,— JCV – NPC diseases – WT1 – HPV WT1: Wilms tumor 1 antigen; HPV: Human papilloma virus 8
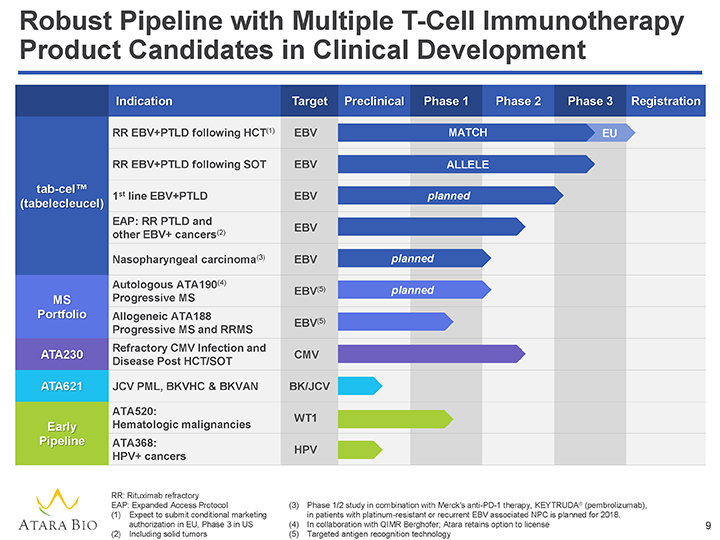
Robust Pipeline with Multiple T-Cell Immunotherapy Product Candidates in Clinical Development Indication Target Preclinical Phas 1 Phase 2 Phase 3 Registration RR EBV+PTLD following HCT(1) EBV MATCH EU RR EBV+PTLD following SOT EBV ALLELE tab cel™ (tabelecleucel) 1st line EBV+PTLD EBV planned EAP: RR PTLD and EBV other EBV+ cancers(2) Nasopharyngeal carcinoma(3) EBV planned Autologous ATA190(4) (5) EBV planned MS Progressive MS Portfolio Allogeneic ATA188 Progressive MS and RRMS EBV(5) Refractory CMV Infection and ATA230 CMV Disease Post HCT/SOT ATA621 JCV PML, BKVHC & BKVAN BK/JCV ATA520: WT1 Early Hematologic malignancies Pipeline ATA368: HPV HPV+ cancers RR: Rituximab refractory EAP: Expanded Access Protocol (3) Phase 1/2 study in combination with Merck’s anti-PD-1 therapy, KEYTRUDA® (pembrolizumab), (1) Expect to submit conditional marketing in patients with platinum-resistant or recurrent EBV associated NPC is planned for 2018. authorization in EU, Phase 3 in US (4) In collaboration with QIMR Berghofer; Atara retains option to license 9 (2) Including solid tumors (5) Targeted antigen recognition technology
A Pioneer in Off-the-Shelf T-Cell Immunotherapy –At an Inflection Point ADVANCING INNOVATIVE ROBUST PIPELINE CLEAR TAB-CEL IN TECHNOLOGY EXPANSION STRATEGIC HEMATOLOGIC & PLATFORM OPPORTUNITIES FOCUS SOLID TUMORS ï,— Proprietaryï,— Two Phase 3ï,— Encouraging early ï,— Key milestones off-the-shelf T-cell EBV+PTLD results in expected in next 18 immunotherapy studies initiated progressive months technologies multiple sclerosisï,— Phase 1/2 NPC ï,— Preparing for PTLD ï,— Versatile PD-1 combo studyï,— CMV commercialization therapeutic planned in 2018ï,— BKV and JCVï,— Leverage power of applications the platform 10
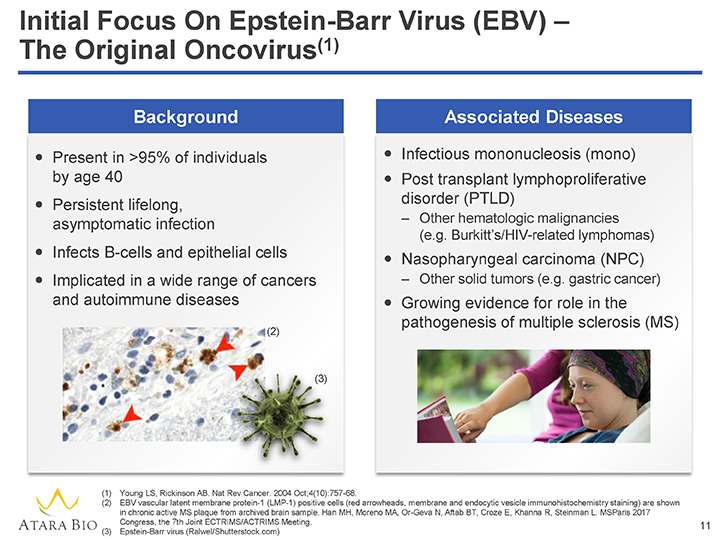
Initial Focus On Epstein-Barr Virus (EBV) –The Original Oncovirus(1) Background Associated Diseases ï,— Present in >95% of individuals ï,— Infectious mononucleosis (mono) by age 40ï,— Post transplant lymphoproliferative ï,— Persistent lifelong, disorder (PTLD) asymptomatic infection – Other hematologic malignancies (e.g. Burkitt’s/HIV-related lymphomas) ï,— Infects B-cells and epithelial cells Nasopharyngeal ï,— carcinoma (NPC)ï,— Implicated in a wide range of cancers – Other solid tumors (e.g. gastric cancer) and autoimmune diseasesï,— Growing evidence for role in the pathogenesis of multiple sclerosis (MS) (2) (3) (1) Young LS, Rickinson AB. Nat Rev Cancer. 2004 Oct;4(10):757-68. (2) EBV vascular latent membrane protein-1 (LMP-1) positive cells (red arrowheads, membrane and endocytic vesicle immunohistochemistry staining) are shown in chronic active MS plaque from archived brain sample. Han MH, Moreno MA, Or-Geva N, Aftab BT, Croze E, Khanna R, Steinman L. MSParis 2017 Congress, the 7th Joint ECTRIMS/ACTRIMS Meeting. 11 (3) Epstein-Barr virus (Ralwel/Shutterstock.com)
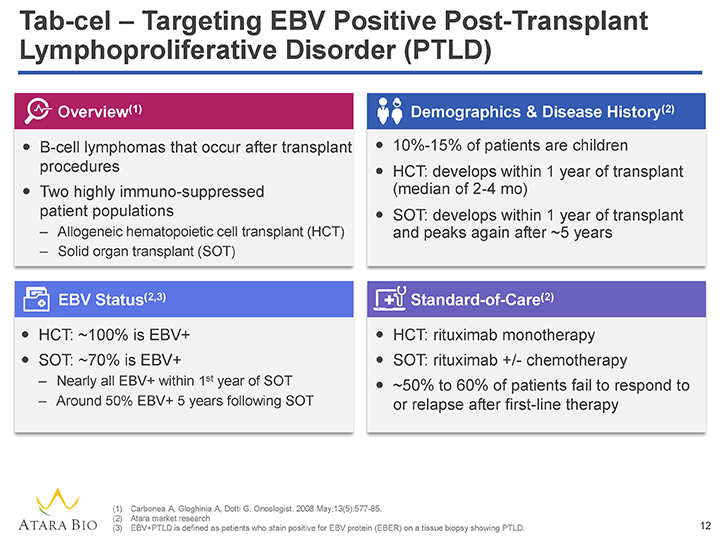
Tab-cel – Targeting EBV Positive Post-Transplant Lymphoproliferative Disorder (PTLD) Overview(1) Demographics & Disease History(2) ï,— B-cell lymphomas that occur after transplant ï,— 10%-15% of patients are children proceduresï,— HCT: develops within 1 year of transplant ï,— Two highly immuno-suppressed (median of 2-4 mo) patient populationsï,— SOT: develops within 1 year of transplant – Allogeneic hematopoietic cell transplant (HCT) and peaks again after ~5 years – Solid organ transplant (SOT) EBV Status(2,3) Standard-of-Care(2) ï,— HCT: ~100% is EBV+ï,— HCT: rituximab monotherapy ï,— SOT: ~70% is EBV+ï,— SOT: rituximab +/- chemotherapy – Nearly all EBV+ within 1st year of SOTï,— ~50% to 60% of patients fail to respond to – Around 50% EBV+ 5 years following SOT or relapse after first-line therapy (1) Carbonea A, Gloghinia A, Dotti G. Oncologist. 2008 May;13(5):577-85. (2) Atara market research (3) EBV+PTLD is defined as patients who stain positive for EBV protein (EBER) on a tissue biopsy showing PTLD. 12
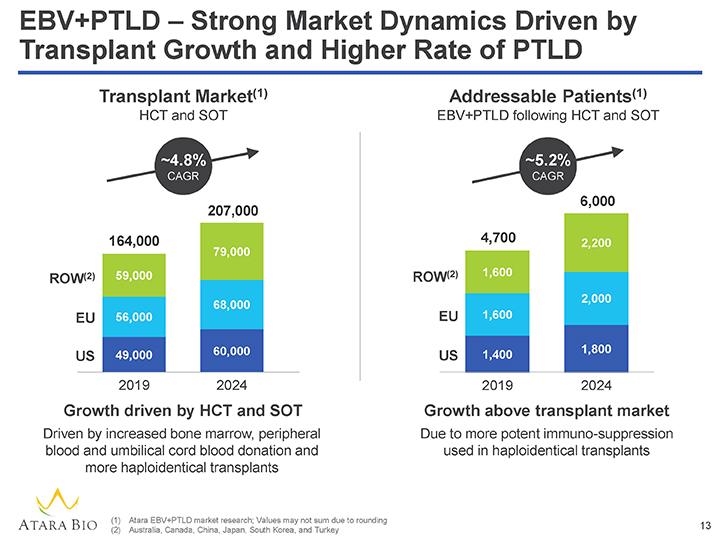
EBV+PTLD – Strong Market Dynamics Driven by Transplant Growth and Higher Rate of PTLD Transplant Market(1) Addressable Patients(1) HCT and SOT EBV+PTLD following HCT and SOT ~4.8% ~5.2% CAGR CAGR 6,000 207,000 164,000 4,700 2,200 79,000 (2) 59,000 ROW(2) 1,600 ROW 2,000 68,000 EU 56,000 EU 1,600 60,000 1,800 US 49,000 US 1,400 2019 2024 2019 2024 Growth driven by HCT and SOT Growth above transplant market Driven by increased bone marrow, peripheral Due to more potent immuno-suppression blood and umbilical cord blood donation and used in haploidentical transplants more haploidentical transplants (1) Atara EBV+PTLD market research; Values may not sum due to rounding (2) Australia, Canada, China, Japan, South Korea, and Turkey 13
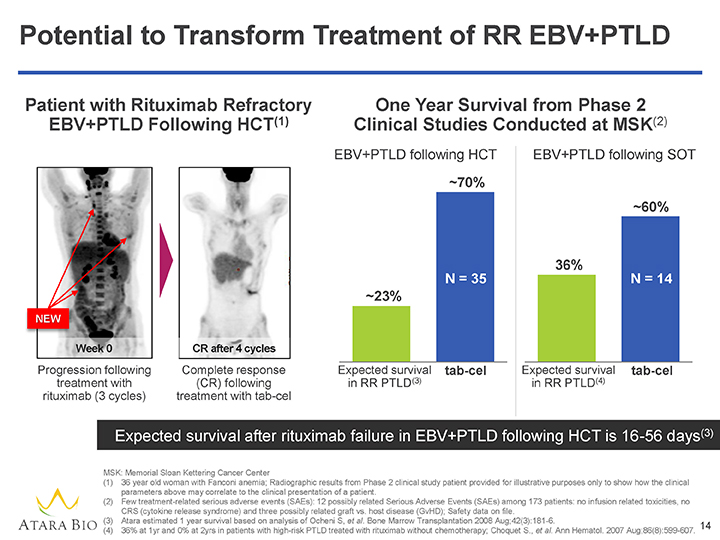
Potential to Transform Treatment of RR EBV+PTLD Patient with Rituximab Refractory One Year Survival from Phase 2 EBV+PTLD Following HCT(1) Clinical Studies Conducted at MSK(2) EBV+PTLD following HCT EBV+PTLD following SOT ~70% ~60% 36% N = 35 N = 14 ~23% NEW Week 0 CR after 4 cycles Progression following Complete response Expected survival tab-cel Expected survival tab-cel treatment with (CR) following in RR PTLD(3) in RR PTLD(4) rituximab (3 cycles) treatment with tab-cel Expected survival after rituximab failure in EBV+PTLD following HCT is 16-56 days(3) MSK: Memorial Sloan Kettering Cancer Center (1) 36 year old woman with Fanconi anemia; Radiographic results from Phase 2 clinical study patient provided for illustrative purposes only to show how the clinical parameters above may correlate to the clinical presentation of a patient. (2) Few treatment-related serious adverse events (SAEs): 12 possibly related Serious Adverse Events (SAEs) among 173 patients: no infusion related toxicities, no CRS (cytokine release syndrome) and three possibly related graft vs. host disease (GvHD); Safety data on file. (3) Atara estimated 1 year survival based on analysis of Ocheni S, et al. Bone Marrow Transplantation 2008 Aug;42(3):181-6. 14 (4) 36% at 1yr and 0% at 2yrs in patients with high-risk PTLD treated with rituximab without chemotherapy; Choquet S., et al. Ann Hematol. 2007 Aug;86(8):599-607.
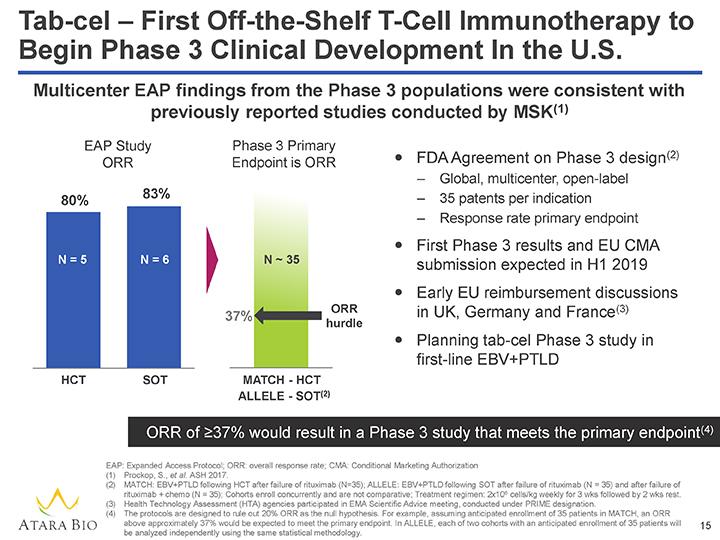
Tab-cel – First Off-the-Shelf T-Cell Immunotherapy to Begin Phase 3 Clinical Development In the U.S. Multicenter EAP findings from the Phase 3 populations were consistent with previously reported studies conducted by MSK(1) EAP Study Phase 3 Primary ï,— FDA Agreement on Phase 3 design(2) ORR Endpoint is ORR – Global, multicenter, open-label 83% – 35 patents per indication 80% – Response rate primary endpoint ï,— First Phase 3 results and EU CMA N = 5 N = 6 N ~ 35 submission expected in H1 2019ï,— Early EU reimbursement discussions ORR in UK, Germany and France(3) 37% hurdle ï,— Planning tab-cel Phase 3 study in first-line EBV+PTLD HCT SOT MATCH—HCT ALLELE—SOT(2) ORR of ³37% would result in a Phase 3 study that meets the primary endpoint(4) EAP: Expanded Access Protocol; ORR: overall response rate; CMA: Conditional Marketing Authorization (1) Prockop, S., et al. ASH 2017. (2) MATCH: EBV+PTLD following HCT after failure of rituximab (N=35); ALLELE: EBV+PTLD following SOT after failure of rituximab (N = 35) and after failure of rituximab + chemo (N = 35); Cohorts enroll concurrently and are not comparative; Treatment regimen: 2x106 cells/kg weekly for 3 wks followed by 2 wks rest. (3) Health Technology Assessment (HTA) agencies participated in EMA Scientific Advice meeting, conducted under PRIME designation. (4) The protocols are designed to rule out 20% ORR as the null hypothesis. For example, assuming anticipated enrollment of 35 patients in MATCH, an ORR above approximately 37% would be expected to meet the primary endpoint. In ALLELE, each of two cohorts with an anticipated enrollment of 35 patients will 15 be analyzed independently using the same statistical methodology.
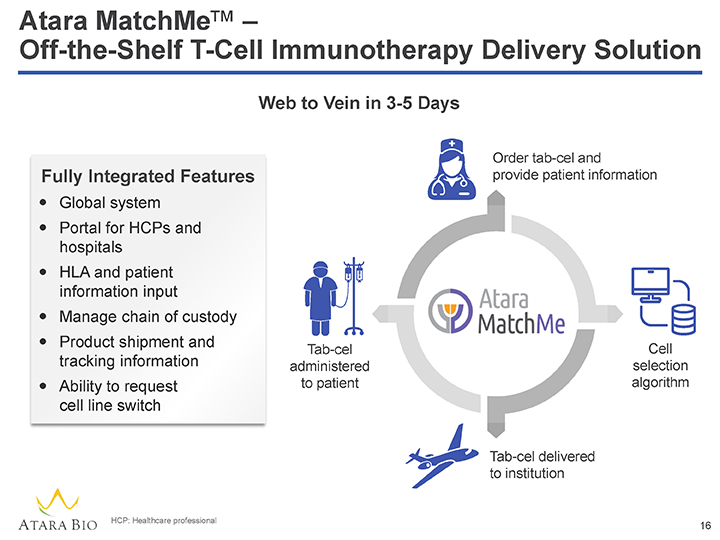
Atara MatchMe™ – Off-the-Shelf T-Cell Immunotherapy Delivery Solution Web to Vein in 3-5 Days Order tab-cel and Fully Integrated Features provide patient information ï,— Global systemï,— Portal for HCPs and hospitalsï,— HLA and patient information inputï,— Manage chain of custodyï,— Product shipment and Tab-cel Cell tracking information administered selection ï,— Ability to request to patient algorithm cell line switch Tab-cel delivered to institution HCP: Healthcare professional 16
Tab-cel – Compelling Value Proposition in EBV+PTLD High and durable response Off-the-shelf data(1) 10%-15% pediatric Low cost of population administration Tab-cel Value Proposition Cost- Repeat dosing & effective therapy(2) cell line switching Few treatment Potential to related serious minimize risk events of graft loss(3) (1) Prockop S, et al., Proc ASCO 2015; Atara data on file. (2) Initial Atara value-based assessment (3) Franke AJ, et al. Proc. ASCO 2017 17
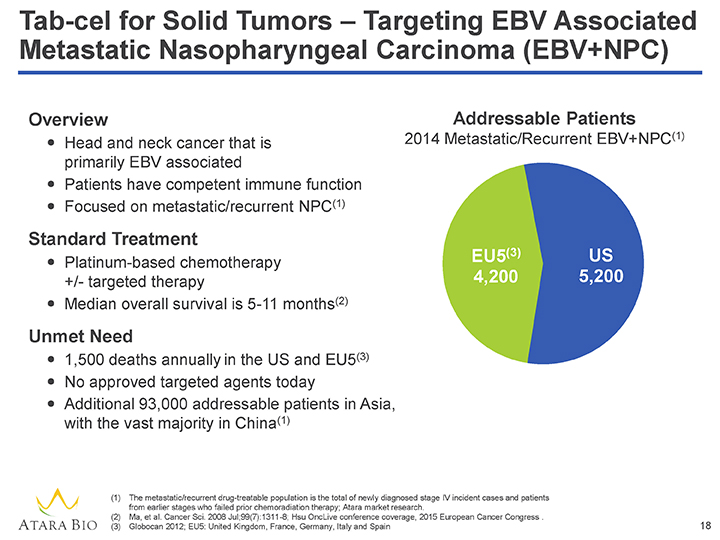
Tab-cel for Solid Tumors – Targeting EBV Associated Metastatic Nasopharyngeal Carcinoma (EBV+NPC) Overview Addressable Patients Head and neck 2014 Metastatic/Recurrent EBV+NPC(1)ï,— cancer that is primarily EBV associatedï,— Patients have competent immune functionï,— Focused on metastatic/recurrent NPC(1) Standard Treatment EU5(3) US ï,— Platinum-based chemotherapy +/- targeted therapy 4,200 5,200ï,— Median overall survival is 5-11 months(2) Unmet Need ï,— 1,500 deaths annuallyin the US and EU5(3)ï,— No approved targeted agents todayï,— Additional 93,000 addressable patients in Asia, with the vast majority in China(1) (1) The metastatic/recurrent drug-treatable population is the total of newly diagnosed stage IV incident cases and patients from earlier stages who failed prior chemoradiation therapy; Atara market research. (2) Ma, et al. Cancer Sci. 2008 Jul;99(7):1311-8; Hsu OncLive conference coverage, 2015 European Cancer Congress . (3) Globocan 2012; EU5: United Kingdom, France, Germany, Italy and Spain 18
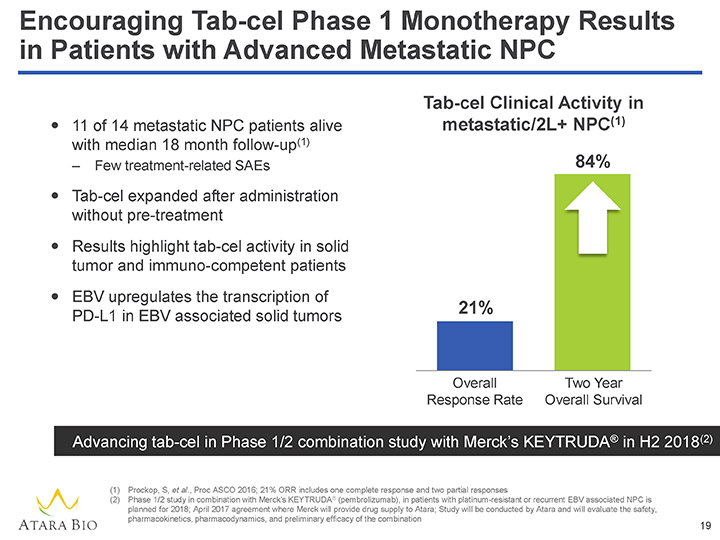
Encouraging Tab-cel Phase 1 Monotherapy Results in Patients with Advanced Metastatic NPC Tab-cel Clinical Activity in ï,— 11 of 14 metastatic NPC patients alive metastatic/2L+ NPC(1) with median 18 month follow-up(1) – Few treatment-related SAEs 84% ï,— Tab-cel expanded after administration without pre-treatmentï,— Results highlight tab-cel activity in solid tumor and immuno-competent patientsï,— EBV upregulates the transcription of 21% PD-L1 in EBV associated solid tumors Overall Two Year Response Rate Overall Survival Advancing tab-cel in Phase 1/2 combination study with Merck’s KEYTRUDA® in H2 2018(2) (1) Prockop, S, et al., Proc ASCO 2016; 21% ORR includes one complete response and two partial responses (2) Phase 1/2 study in combination with Merck’s KEYTRUDA® (pembrolizumab), in patients with platinum-resistant or recurrent EBV associated NPC is planned for 2018; April 2017 agreement where Merck will provide drug supply to Atara; Study will be conducted by Atara and will evaluate the safety, pharmacokinetics, pharmacodynamics, and preliminary efficacy of the combination 19
A Pioneer in Off-the-Shelf T-Cell Immunotherapy –At an Inflection Point ADVANCING INNOVATIVE ROBUST PIPELINE CLEAR TAB-CEL IN TECHNOLOGY EXPANSION STRATEGIC HEMATOLOGIC & PLATFORM OPPORTUNITIES FOCUS SOLID TUMORS ï,— Proprietaryï,— Two Phase 3ï,— Encouraging early ï,— Key milestones off-the-shelf T-cell EBV+PTLD results in expected in next 18 immunotherapy studies initiated progressive months technologies multiple sclerosisï,— Phase 1/2 NPC ï,— Preparing for PTLD ï,— Versatile PD-1 combo studyï,— CMV commercialization therapeutic planned in 2018ï,— BKV and JCVï,— Leverage power of applications the platform 20
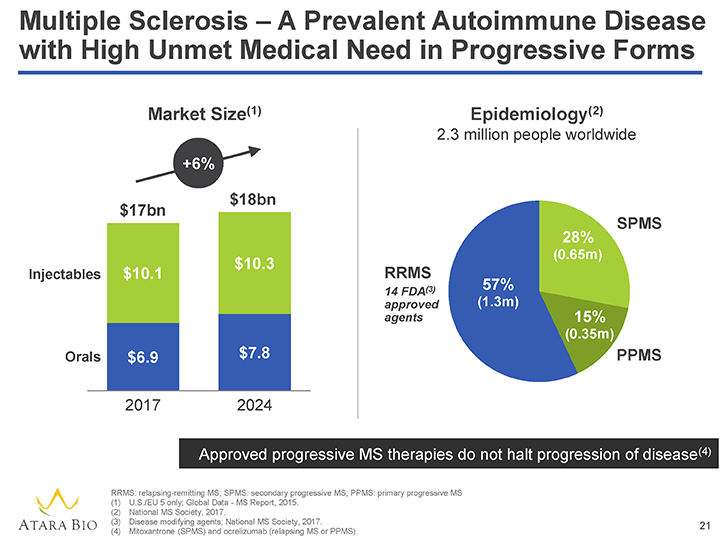
Multiple Sclerosis – A Prevalent Autoimmune Disease with High Unmet Medical Need in Progressive Forms Market Size(1) Epidemiology(2) 2.3 million people worldwide +6% $18bn $17bn 28% SPMS (0.65m) $10.3 Injectables $10.1 RRMS (3) 57% 14 FDA approved (1.3m) agents 15% (0.35m) Orals $6.9 $7.8 PPMS 2017 2024 Approved progressive MS therapies do not halt progression of disease(4) RRMS: relapsing-remitting MS; SPMS: secondary progressive MS; PPMS: primary progressive MS (1) U.S./EU 5 only; Global Data—MS Report, 2015. (2) National MS Society, 2017. (3) Disease modifying agents; National MS Society, 2017. 21 (4) Mitoxantrone (SPMS) and ocrelizumab (relapsing MS or PPMS).
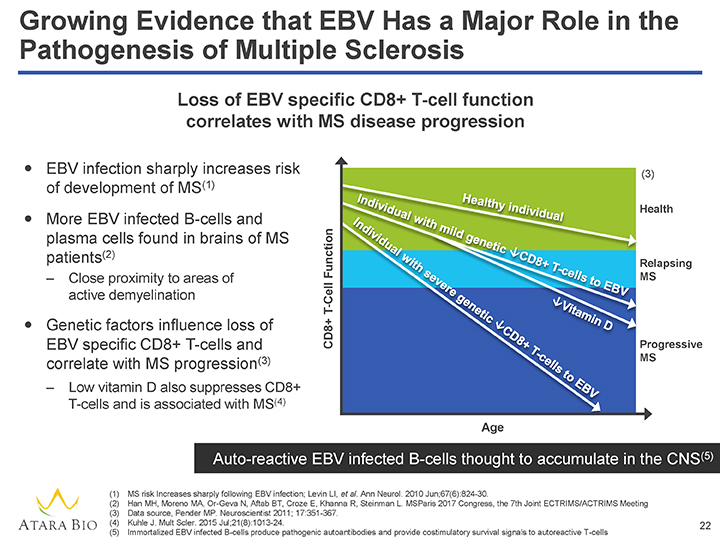
Growing Evidence that EBV Has a Major Role in the Pathogenesis of Multiple Sclerosis Loss of EBV specific CD8+ T-cell function correlates with MS disease progression ï,— EBV infection sharply increases risk (3) of development of MS(1) ealth ï,— More EBV infected B-cells and plasma cells found in brains of MS Function patients(2) elapsing – Close proximity to areas of MS active demyelination T-Cell ï,— Genetic factors influence loss of CD8+ EBV specific CD8+ T-cells and Progressive correlate with MS progression(3) MS – Low vitamin D also suppresses CD8+ T-cells and is associated with MS(4) Age Auto-reactive EBV infected B-cells thought to accumulate in the CNS(5) (1) MS risk Increases sharply following EBV infection; Levin LI, et al. Ann Neurol. 2010 Jun;67(6):824-30. (2) Han MH, Moreno MA, Or-Geva N, Aftab BT, Croze E, Khanna R, Steinman L. MSParis 2017 Congress, the 7th Joint ECTRIMS/ACTRIMS Meeting (3) Data source, Pender MP. Neuroscientist 2011; 17:351-367. (4) Kuhle J. Mult Scler. 2015 Jul;21(8):1013-24. 22 (5) Immortalized EBV infected B-cells produce pathogenic autoantibodies and provide costimulatory survival signals to autoreactive T-cells
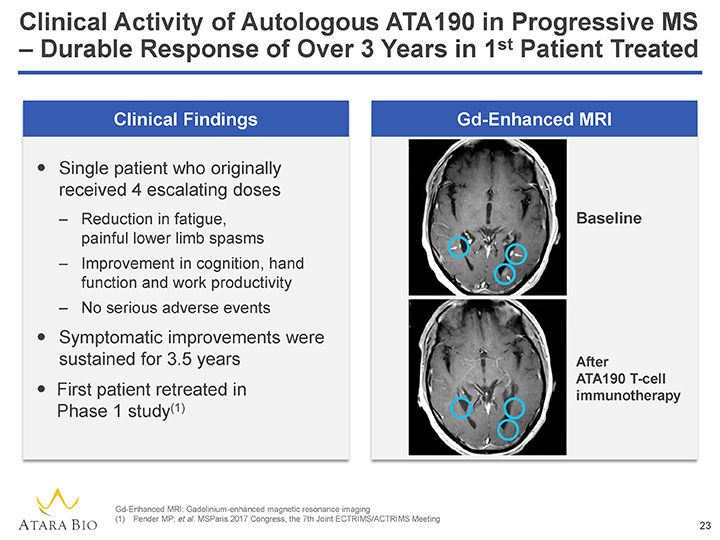
Clinical Activity of Autologous ATA190 in Progressive MS – Durable Response of Over 3 Years in 1st Patient Treated Clinical Findings Gd-Enhanced MRI ï,— Single patient who originally received 4 escalating doses – Reduction in fatigue, Baseline painful lower limb spasms – Improvement in cognition, hand function and work productivity – No serious adverse events ï,— Symptomatic improvements were sustained for 3.5 years After ATA190 T-cell ï,— First patient retreated in immunotherapy Phase 1 study(1) Gd-Enhanced MRI: Gadolinium-enhanced magnetic resonance imaging (1) Pender MP, et al. MSParis 2017 Congress, the 7th Joint ECTRIMS/ACTRIMS Meeting 23
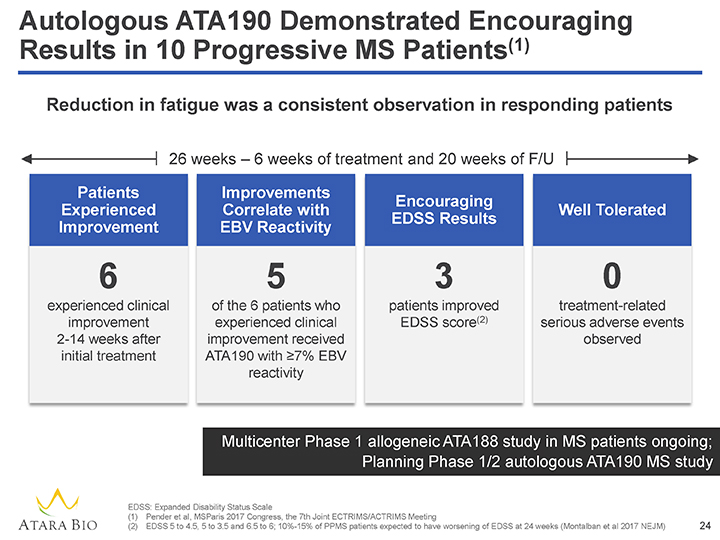
Autologous ATA190 Demonstrated Encouraging Results in 10 Progressive MS Patients(1) Reduction in fatigue was a consistent observation in responding patients 26 weeks – 6 weeks of treatment and 20 weeks of F/U Patients Improvements Encouraging Experienced Correlate with Well Tolerated EDSS Results Improvement EBV Reactivity 6 5 3 0 experienced clinical of the 6 patients who patients improved treatment-related improvement experienced clinical EDSS score(2) serious adverse events 2-14 weeks after improvement received observed initial treatment ATA190 with ³7% EBV reactivity Multicenter Phase 1 allogeneic ATA188 study in MS patients ongoing; Planning Phase 1/2 autologous ATA190 MS study EDSS: Expanded Disability Status Scale (1) Pender et al, MSParis 2017 Congress, the 7th Joint ECTRIMS/ACTRIMS Meeting (2) EDSS 5 to 4.5, 5 to 3.5 and 6.5 to 6; 10%-15% of PPMS patients expected to have worsening of EDSS at 24 weeks (Montalban et al 2017 NEJM) 24
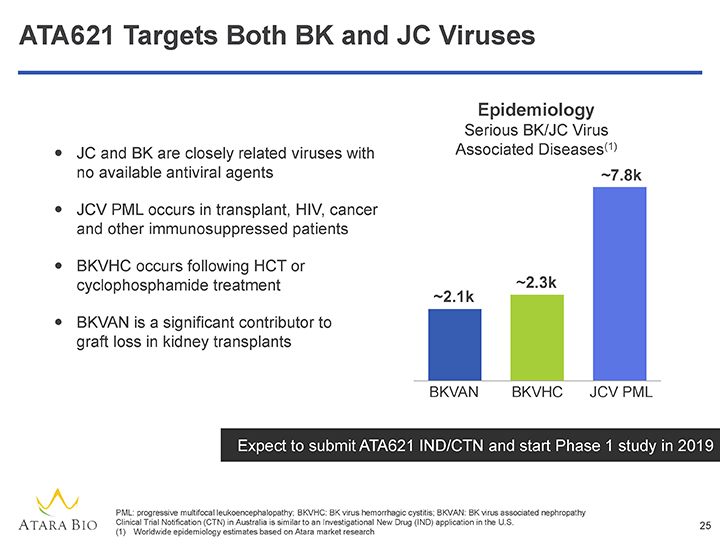
ATA621 Targets Both BK and JC Viruses Epidemiology Serious BK/JC Virus ï,— JC and BK are closely related viruses with Associated Diseases(1) no available antiviral agents ~7.8kï,— JCV PML occurs in transplant, HIV, cancer and other immunosuppressed patients ï,— BKVHC occurs following HCT or cyclophosphamide treatment ~2.1k ~2.3kï,— BKVAN is a significant contributor to graft loss in kidney transplants BKVAN BKVHC JCV PML Expect to submit ATA621 IND/CTN and start Phase 1 study in 2019 PML: progressive multifocal leukoencephalopathy; BKVHC: BK virus hemorrhagic cystitis; BKVAN: BK virus associated nephropathy Clinical Trial Notification (CTN) in Australia is similar to an Investigational New Drug (IND) application in the U.S. 25 (1) Worldwide epidemiology estimates based on Atara market research
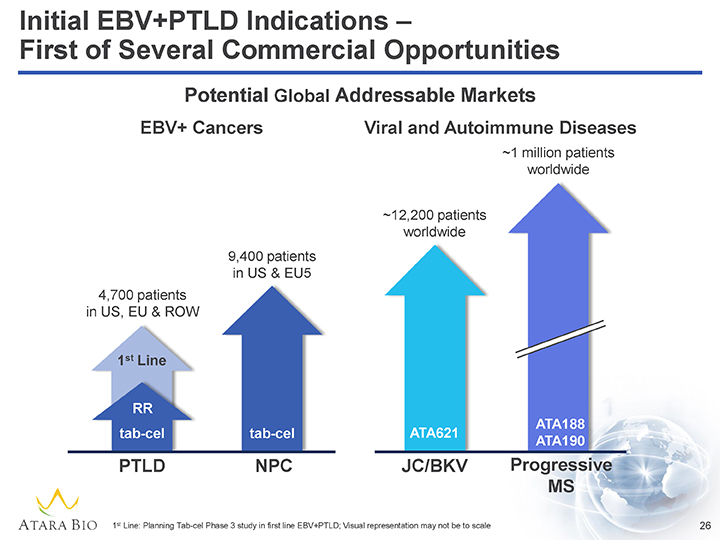
Initial EBV+PTLD Indications – First of Several Commercial Opportunities Potential Global Addressable Markets EBV+ Cancers Viral and Autoimmune Diseases ~1 million patients worldwide ~12,200 patients worldwide 9,400 patients in US & EU5 4,700 patients in US, EU & ROW 1st Line RR ATA188 tab-cel tab-cel ATA621 ATA190 PTLD NPC JC/BKV Progressive MS 1st Line: Planning Tab-cel Phase 3 study in first line EBV+PTLD; Visual representation may not be to scale 26
Executed on Our 2017 Objectives Initiated tab-cel MATCH and ALLELE Phase 3 studies in rituximab refractory EBV+PTLD Presented positive tab-cel EAP EBV+PTLD results Started pre-commercial preparation for planned tab-cel EU CMA submission Announced collaboration with Merck to support Phase 1/2 study of tab-cel in combination with KEYTRUDA® for NPC Initiated allogeneic ATA188 Phase 1 progressive MS study Presented positive autologous ATA190 Phase 1 results in patients with progressive MS 27
A Pioneer in Off-the-Shelf T-Cell Immunotherapy –At an Inflection Point ADVANCING INNOVATIVE ROBUST PIPELINE CLEAR TAB-CEL IN TECHNOLOGY EXPANSION STRATEGIC HEMATOLOGIC & PLATFORM OPPORTUNITIES FOCUS SOLID TUMORS ï,— Proprietaryï,— Two Phase 3ï,— Encouraging early ï,— Key milestones off-the-shelf T-cell EBV+PTLD results in expected in next 18 immunotherapy studies initiated progressive months technologies multiple sclerosisï,— Phase 1/2 NPC ï,— Preparing for PTLD ï,— Versatile PD-1 combo studyï,— CMV commercialization therapeutic planned in 2018ï,— BKV and JCVï,— Leverage power of applications the platform 28
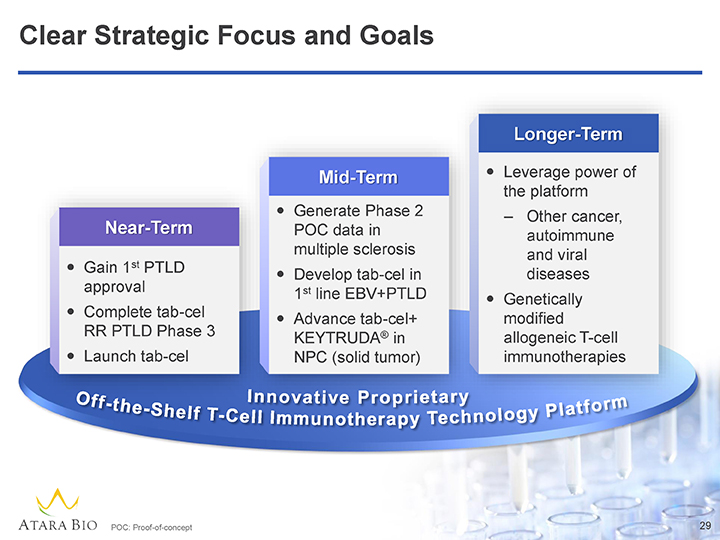
Clear Strategic Focus and Goals Long Term Mid Termï,— Leverage power of the platformï,— Generate Phase 2 – Other cancer, Ne Term POC data in multiple sclerosis autoimmune and viral ï,— Gain 1st PTLD ï,— Develop tab-cel in diseases approval 1st line EBV+PTLDï,— Genetically ï,— Complete tab-cel modified ï,— Advance tab-cel+ RR PTLD Phase 3 ® allogeneic T-cell KEYTRUDA in ï,— Launch tab-cel NPC (solid tumor) immunotherapies POC: Proof-of-concept 29
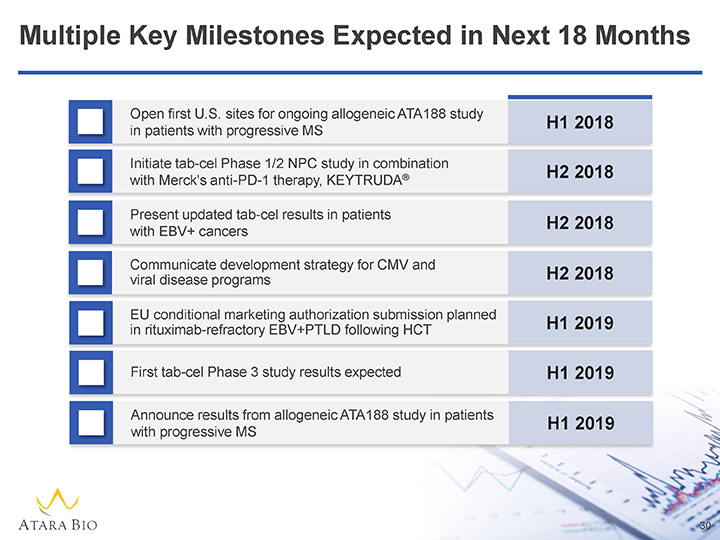
Multiple Key Milestones Expected in Next 18 Months Open first U.S. sites for ongoing allogeneic ATA188 study H1 2018 in patients with progressive MS Initiate tab-cel Phase 1/2 NPC study in combination ® H2 2018 with Merck’s anti-PD-1 therapy, KEYTRUDA Present updated tab-cel results in patients H2 2018 with EBV+ cancers Communicate development strategy for CMV and viral disease programs H2 2018 EU conditional marketing authorization submission planned in rituximab-refractory EBV+PTLD following HCT H1 2019 First tab-cel Phase 3 study results expected H1 2019 Announce results from allogeneic ATA188 study in patients H1 2019 with progressive MS 30
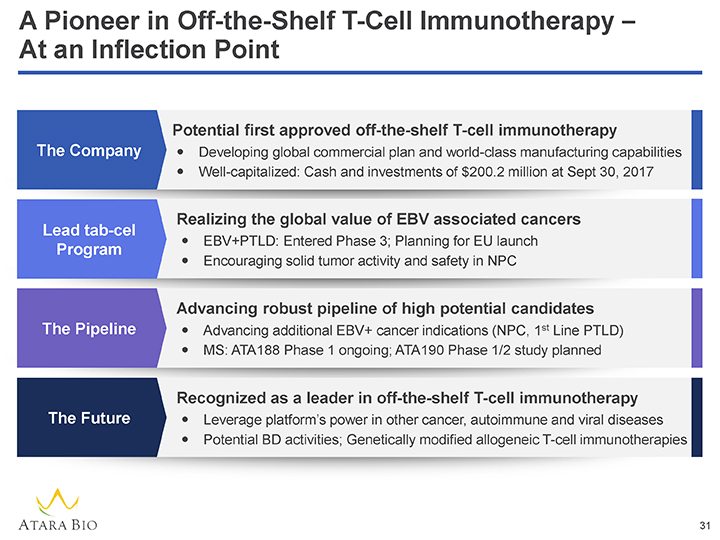
A Pioneer in Off-the-Shelf T-Cell Immunotherapy –At an Inflection Point Potential first approved off-the-shelf T-cell immunotherapy The Companyï,— Developing global commercial plan and world-class manufacturing capabilitiesï,— Well-capitalized: Cash and investments of $200.2 million at Sept 30, 2017 Realizing the global value of EBV associated cancers Lead tab-cel ï,— EBV+PTLD: Entered Phase 3; Planning for EU launch Program ï,— Encouraging solid tumor activity and safety in NPC Advancing robust pipeline of high potential candidates The Pipelineï,— Advancing additional EBV+ cancer indications (NPC, 1st Line PTLD)ï,— MS: ATA188 Phase 1 ongoing; ATA190 Phase 1/2 study planned Recognized as a leader in off-the-shelf T-cell immunotherapy The Futureï,— Leverage platform’s power in other cancer, autoimmune and viral diseases ï,— Potential BD activities; Genetically modified allogeneic T-cell immunotherapies 31