
As filed with the Securities and Exchange Commission on June 29, 2015.
Registration No. 333-
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM S-1
REGISTRATION STATEMENT
UNDER
THE SECURITIES ACT OF 1933
ATARA BIOTHERAPEUTICS, INC.
(Exact name of Registrant as specified in its charter)
| Delaware | 2836 | 46-0920988 | ||
| (State or other jurisdiction of incorporation or organization) |
(Primary Standard Industrial Classification Code Number) |
(I.R.S. Employer Identification Number) |
701 Gateway Blvd., Suite 200
South San Francisco, California 94080
(650) 278-8930
(Address, including zip code and telephone number, of Registrant’s principal executive offices)
Isaac E. Ciechanover, M.D.
Chief Executive Officer
Atara Biotherapeutics, Inc.
701 Gateway Blvd., Suite 200
South San Francisco, California 94080
(650) 278-8930
(Name, address, including zip code and telephone number, including area code, of agent for service)
Copies to:
| Kenneth L. Guernsey Jodie M. Bourdet Cooley LLP 101 California Street, 5th Floor San Francisco, California 94111 (415) 693-2000 |
Bruce K. Dallas Davis Polk & Wardwell LLP 1600 El Camino Real Menlo Park, California 94025 (650) 752-2000 |
Approximate date of commencement of proposed sale to the public: As soon as practicable after the effective date of this registration statement.
If any of the securities being registered on this Form are to be offered on a delayed or continuous basis pursuant to Rule 415 under the Securities Act, check the following box. ¨
If this Form is filed to register additional securities for an offering pursuant to Rule 462(b) under the Securities Act, please check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ¨
If this Form is a post-effective amendment filed pursuant to Rule 462(c) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ¨
If this Form is a post-effective amendment filed pursuant to Rule 462(d) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ¨ | Accelerated filer | ¨ | |||
| Non-accelerated filer | þ (Do not check if a smaller reporting company) | Smaller reporting company | ¨ |
CALCULATION OF REGISTRATION FEE
|
| ||||
| Title of securities to be registered | Proposed maximum aggregate offering price(1)(2) |
Amount of registration fee | ||
| Common Stock, par value $0.0001 per share |
$143,750,000 | $16,704 | ||
|
| ||||
|
| ||||
| (1) | Includes the offering price of any additional shares that the underwriters have the option to purchase from the Registrant. |
| (2) | Estimated solely for the purpose of computing the registration fee pursuant to Rule 457(o) under the Securities Act of 1933, as amended. |
The Registrant hereby amends this Registration Statement on such date or dates as may be necessary to delay its effective date until the Registrant shall file a further amendment which specifically states that this Registration Statement shall thereafter become effective in accordance with Section 8(a) of the Securities Act of 1933, as amended, or until the Registration Statement shall become effective on such date as the Securities and Exchange Commission acting pursuant to said Section 8(a), may determine.
The information in this preliminary prospectus is not complete and may be changed. These securities may not be sold until the registration statement filed with the Securities and Exchange Commission is effective. This preliminary prospectus is not an offer to sell nor does it seek an offer to buy these securities in any jurisdiction where the offer or sale is not permitted.
Subject to Completion. Dated June 29, 2015.
$125,000,000
Common Stock
We are offering $125,000,000 of shares of our common stock or, assuming a public offering price of $52.62 per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on June 26, 2015, 2,375,522 shares of our common stock. Our common stock is listed on The Nasdaq Global Select Market under the symbol “ATRA.”
We are an “emerging growth company” under applicable Securities and Exchange Commission rules and are subject to reduced public company reporting requirements.
Investing in our common stock involves a high degree of risk. See “Risk Factors” beginning on page 12 to read about factors you should consider before buying shares of our common stock.
Neither the Securities and Exchange Commission nor any other regulatory body has approved or disapproved of these securities or passed upon the accuracy or adequacy of this prospectus. Any representation to the contrary is a criminal offense.
| Per Share | Total | |||||||
| Public offering price |
$ | $ | ||||||
| Underwriting discounts and commissions(1) |
$ | $ | ||||||
| Proceeds to us, before expenses |
$ | $ | ||||||
| (1) | We refer you to “Underwriting” beginning on page 132 for additional information regarding total underwriting compensation. |
We have granted the underwriters an option to purchase up to an additional $18,750,000 of shares of common stock at the public offering price, less underwriting discounts and commissions.
The underwriters expect to deliver the shares against payment in New York, New York on , 2015.
| Goldman, Sachs & Co. | Citigroup |
| Canaccord Genuity | JMP Securities | SunTrust Robinson Humphrey | ||
Prospectus dated , 2015
| Page | ||||
| 1 | ||||
| 10 | ||||
| 12 | ||||
| Special Note Regarding Forward-Looking Statements and Industry Data |
52 | |||
| 54 | ||||
| 55 | ||||
| 56 | ||||
| 57 | ||||
| 58 | ||||
| 59 | ||||
| 114 | ||||
| 118 | ||||
| 121 | ||||
| 126 | ||||
| Material US Federal Income Tax Consequences to Non-US Holders of Our Common Stock |
128 | |||
| 132 | ||||
| 138 | ||||
| 138 | ||||
| 138 | ||||
| 139 | ||||
We have not authorized anyone to provide you with any information or to make any representation, other than those contained or incorporated by reference in this prospectus or in any free writing prospectus we have prepared. We take no responsibility for, and provide no assurance as to the reliability of, any other information that others may give you. This prospectus is an offer to sell only the shares offered hereby, but only in circumstances and in jurisdictions where it is lawful to so do. The information contained or incorporated by reference in this prospectus is accurate only as of its date, regardless of the time of delivery of this prospectus or of any sale of our common stock.
Neither we nor any of the underwriters have done anything that would permit this offering or possession or distribution of this prospectus in any jurisdiction where action for that purpose is required, other than the United States. You are required to inform yourself about, and to observe any restrictions relating to, this offering and the distribution of this prospectus.
Atara, Atara Biotherapeutics, the Atara logo and other trade names, trademarks or service marks of Atara appearing in this prospectus are the property of Atara. Trade names, trademarks and service marks of other companies appearing in this prospectus are the property of their respective holders.
This summary highlights information contained or incorporated by reference in this prospectus and does not contain all of the information that you should consider in making your investment decision. Before investing in our common stock, you should read the entire prospectus carefully, including the section titled “Risk Factors” and the information in our filings with the Securities and Exchange Commission, or SEC, incorporated by reference in this prospectus. Unless the context suggests otherwise, references in this prospectus to “Atara,” “Atara Biotherapeutics,” “we,” “us” and “our” refer to Atara Biotherapeutics, Inc. and, where appropriate, its subsidiaries.
Atara Biotherapeutics, Inc.
We are a clinical-stage biopharmaceutical company focused on developing novel therapeutics for serious unmet medical needs, with an initial focus on muscle wasting conditions, oncology and viral-associated diseases. We have two groups of product candidates: molecularly targeted biologics and allogeneic, or third-party derived, antigen-specific T-cells, a type of white blood cell. Our molecularly targeted product candidates are biologics that inhibit myostatin and activin, members of the Transforming Growth Factor-Beta, or TGF-ß, protein superfamily, which play roles in the growth and maintenance of muscle and many other body tissues. Our lead molecularly targeted product candidate, PINTA 745, is in a Phase 2 clinical trial for protein energy wasting, a condition affecting many end-stage renal disease patients. Our second molecularly targeted product candidate is STM 434. We commenced a Phase 1 clinical study of STM 434 for ovarian cancer and other solid tumors in 2014. We have five additional molecularly targeted product candidates that modulate the TGF-ß pathway in preclinical development. Our T-cell product candidates arise from a platform technology designed to produce off-the-shelf, partially human leukocyte antigen matched cellular therapeutics. We licensed these product candidates from Memorial Sloan Kettering Cancer Center, or MSK, in June 2015. Our initial T-cell product candidates target viral- or cancer-specific antigens and are designed to harness the body’s immune system to counteract specific viral infections and cancers. Our most advanced T-cell product candidate, EBV-CTL, is in Phase 2 clinical trials for malignancies associated with Epstein-Barr Virus, including EBV-associated lymphoproliferative diseases, or EBV-LPD. EBV-LPD is a cancer affecting some patients who have received an allogeneic hematopoietic cell transplant, or HCT, or a solid organ transplant, or SOT, or are otherwise immunocompromised. In February 2015, the US Food and Drug Administration, or the FDA, granted Breakthrough Therapy designation for EBV-CTL in the treatment of rituximab-refractory EBV-LPD after HCT, commonly known as bone marrow transplant. Our second T-cell product candidate, CMV-CTL, is in Phase 2 clinical trials for cytomegalovirus, or CMV, an infection that occurs in some patients who have received an HCT, SOT, or are otherwise immunocompromised. Our third T-cell product candidate, WT1-CTL, targets cancers expressing the antigen Wilms Tumor 1 and is currently in Phase 1 clinical studies.
Our Novel Approach to Treat Protein Energy Wasting in ESRD Patients: PINTA 745
Our lead molecularly targeted product candidate, PINTA 745, is a peptibody that binds to and inhibits myostatin, a protein that down regulates muscle growth and maintenance. In a Phase 1 study, PINTA 745 was found to increase muscle mass compared to placebo after one month of weekly dosing, an increase that was statistically significant, indicating that it is more likely than not that the benefit observed in the study was due to drug treatment rather than chance. We are enrolling a US-based Phase 2 clinical trial to further establish the role of PINTA 745 in building muscle mass, as well as to collect data from corresponding functional muscle tests. This trial is being conducted in patients with end-stage renal disease, or ESRD, who are also suffering from protein-energy wasting, or PEW, a condition characterized by muscle wasting, inflammation and malnutrition.
1
PEW is a major complication of ESRD. A recent study we completed with DaVita Clinical Research, a division of DaVita Healthcare Partners Inc., concluded that more than half of the patients in DaVita’s dialysis population met the conditions for PEW and, in comparison to the rest of the group, exhibited worse morbidity and mortality. Based on data from the US Renal Data System, we estimate that the current total US dialysis population, excluding patients who had successfully received kidney transplants, is 460,000 patients. Of these patients, we estimate that approximately 250,000 patients suffer from PEW. Worldwide, we believe that more than 800,000 patients suffer from PEW.
There is currently no approved therapy for patients suffering from PEW. We believe PINTA 745 is the only therapeutic in clinical development to treat this patient population.
In clinical studies conducted of PINTA 745 in men with prostate cancer and in mouse studies in a model of chronic kidney disease, or CKD, conducted with PINTA 745/s, a version of PINTA 745 that was customized for use in mice, several properties well suited for a potential therapeutic for PEW were observed, including:
| • | Reversing muscle loss — PINTA 745 not only stopped muscle wasting, it significantly increased muscle mass after four weeks of treatment. |
| • | Anti-inflammatory properties — In an animal model of renal disease, PINTA 745/s exhibited significant anti-inflammatory properties, a factor that we believe will be important due to the critical role that inflammation plays in PEW and the overall declining health of ESRD patients. |
| • | Dosing schedule — PINTA 745 is dosed weekly, which conveniently aligns with dialysis treatment schedules. |
Our ongoing US-based Phase 2 trial is a 48-patient, randomized, double-blind, placebo-controlled trial that, in addition to providing us with assessments of change in muscle mass and muscle strength, will give us insight into potential additional markets for PINTA 745. These could include: orthopedic indications; inflammation and inflammatory diseases; age-related sarcopenia, or loss of muscle; and cancer cachexia, a syndrome of progressive weight loss. In each of these conditions, muscle loss prevention, muscle growth and reduction in inflammation resulting from treatment with PINTA 745 could lead to improved physical function and therefore better outcomes. As of June 30, 2015, we had enrolled of the planned 48 patients, and we expect to release preliminary top-line data from this Phase 2 clinical trial in the fourth quarter of 2015.
Our Novel Approach to Treat Ovarian Cancer: STM 434
Our second molecularly targeted product candidate, STM 434, is in a Phase 1 clinical study that will enroll approximately 66 patients with ovarian cancer and other solid tumors. STM 434 is a soluble ActR2B receptor that binds Activin A. Activin has been shown to be involved in the growth and proliferation of ovarian cancer and other tumors, with published evidence of its role at both the genetic, or messenger RNA, and protein levels. Activin expression is one of a few biomarkers associated with larger tumor volume and poorer outcomes, including shortened survival, in a variety of tumors including ovarian tumors. Published data has shown that serum Activin A levels in ovarian cancer subjects are elevated in relation to levels in normal subjects. We are testing the potential use of Activin A as a biomarker in our Phase 1 clinical study.
Ovarian cancer is the fifth leading cause of cancer death in women in the United States. According to the National Cancer Institute, there were an estimated 22,240 new ovarian cancer cases and 14,030 ovarian cancer deaths in the United States in 2013. Surgery and cytotoxic chemotherapies are widely used to treat ovarian cancer; however, the outcomes have changed little in 40 years. The
2
proportion of all ovarian cancer patients surviving five years after diagnosis was only 44% based on the National Cancer Institute SEER database for women diagnosed from 2003 to 2009.
Some subtypes of ovarian tumors respond even more poorly to treatment than others and represent opportunities where drug development could be accelerated. In particular, clear cell and granulosa cell tumors are considered resistant to chemotherapy. Our preclinical experiments in animal models of these subtypes indicate that binding Activin A with a soluble receptor could significantly reduce tumor proliferation, reduce tumor volume and potentially increase survival. We believe that novel therapies for clear cell and granulosa cell tumors could qualify for Breakthrough Therapy designation, an FDA process designed to accelerate the development and review of drugs intended to treat a serious condition when early studies show that the drug may be substantially better than current treatment. Based on its mechanism of action, we also believe that STM 434 has the potential to be the first product to target tumor growth and proliferation through the inhibition of Activin A.
Both PINTA 745 and STM 434 are novel molecules with well-characterized mechanisms of action. They were developed initially, along with our five other in-licensed molecularly targeted biologic programs, at Amgen Inc., or Amgen. Taken together, we believe these unique product candidates constitute a pipeline of biologics that have benefited from years of investment, resulting in a large patent portfolio, broad preclinical testing and, in the case of PINTA 745, promising clinical results. We are evaluating the remaining five product candidates to determine the best path forward. Where appropriate, we intend to conduct preclinical studies and file investigational new drug applications, or INDs, with the FDA for these candidates. For example, we are conducting IND-enabling manufacturing and preclinical studies for ATA 842, a humanized antibody targeting myostatin.
T-Cell Therapy for Cancer and Viral-Associated Diseases: MSK T-Cell Programs
T-cells are a critical component of the body’s immune system and can be harnessed to counteract viral infections and some cancers. By focusing the T-cells on specific proteins involved in cancers and infections, the power of the immune system can be employed to combat these diseases. In June 2015, we exclusively licensed from MSK worldwide rights to three clinical stage T-cell product candidates. We also have an exclusive option to exclusively license from MSK worldwide rights to certain other T-cell programs that are discovered or developed by MSK pursuant to sponsored research funded by us.
Our most advanced T-cell product candidate, EBV-CTL, is in Phase 2 clinical trials for the treatment of EBV-associated malignancies. EBV is the virus that causes mononucleosis and is associated with a number of more severe diseases, including certain malignancies and neurologic conditions, such as multiple sclerosis. EBV-CTL received Breakthrough Therapy designation from the FDA in February 2015 for the treatment of patients with rituximab-refractory EBV-LPD after HCT, based on data from two separate clinical trials conducted by MSK. We recently met with the FDA to discuss late-stage development to support a potential approval in this indication. Based on guidance from the FDA, we intend to conduct a pivotal study in rituximab-refractory EBV-LPD after HCT and expect to submit a special protocol assessment for this pivotal study. In addition, we had preliminary discussions with the FDA regarding late-stage development in the setting of rituximab-refractory EBV-LPD after SOT, and we will be incorporating this feedback into our subsequent development plans in this indication.
Our second T-cell product candidate, CMV-CTL, targets cytomegalovirus. CMV infection can result in blindness, illness or death, depending on the tissue it affects in those with weakened immune systems. CMV is also associated with certain malignancies, including glioblastoma multiforme, or GBM. CMV-CTL is currently being investigated in Phase 2 clinical trials sponsored and conducted by MSK for CMV infections that occur in some patients who have received an HCT.
3
Our third clinical stage T-cell product candidate, WT1-CTL, targets Wilms Tumor 1, or WT1. Abnormal expression of WT1 is seen in a variety of hematologic and solid tumors, including multiple myeloma, acute myeloid leukemia and ovarian cancer. This product candidate is currently in Phase 1 clinical trials sponsored and conducted by MSK.
Clinical experience with our T-cell product candidates is broad, including in immunocompromised states, as well as in solid and hematologic malignancies. Selected data from clinical studies of our three T-cell product candidates are summarized in the table below.
| T-Cell Program | Stage | Indication | Recent Clinical Data Highlights |
Number of Patients Who Received Prior Therapy |
Historical Outcomes Data | |||||
|
EBV-CTL |
Phase 2 clinical trials | EBV lymphoma (EBV-LPD) following allogeneic hematopoietic cell transplantation (HCT) from bone marrow or cord blood | 62% response rate in 26 patients treated with EBV-CTL derived from primary HCT donors with 16 complete responses (CR) and zero partial responses (PR) | 13 of 26 received prior rituximab | Historical median survival in rituximab refractory patients is 16-56 days | |||||
| 65% response rate in 34 patients treated with EBV-CTL derived from third-party donor, with 19 CR and three PRs; one-year overall survival (OS) range 56.3-71.8%; two-year OS range 46.9-63.8% |
All received prior rituximab | |||||||||
| EBV-LPD following solid organ transplantation (SOT) | 62% response rate in 13 patients treated with third-party derived EBV-CTL with one CR, seven PRs; two-year OS of 57.7% |
All received prior rituximab; 11 of 13 had received prior chemotherapy; 12 of 13 patients had high risk disease | Historical data show 33% OS at two years in patients with incomplete response to rituximab | |||||||
|
CMV-CTL |
Phase 2 clinical trials | Post-HCT antiviral drug resistant CMV viremia (high viral count) and symptomatic CMV disease | 64% response rate in 25 CMV viremia patients treated with third-party derived CMV-CTL, with nine CRs and seven PRs; 67% response rate in nine CMV disease patients, with five CRs and one PR |
All received prior antiviral therapy; median of four prior therapies including experimental therapies | Uncontrolled CMV disease leads to high rates of morbidity and mortality (for example, CMV pneumonitis confers a four-fold higher risk of death) | |||||
|
WT1-CTL |
Phase 1 clinical studies | Various cancers, including acute myeloid leukemia (AML), multiple myeloma | Data not yet available | Not Applicable | Not Applicable |
4
We are focusing our initial development and regulatory activities on EBV-CTL in the post-HCT and post-SOT setting and CMV-CTL in the post-HCT setting, rare conditions which we believe offer a rapid path to marketing approvals, if supported by additional clinical data. However, we intend to explore the clinical utility of our T-cell product candidates in other more prevalent disease states.
We anticipate that our T-cell technology platform will have utility beyond the current set of targets to which it has been directed. We and MSK have agreed to collaborate on further research to develop additional cellular therapies, which may include T-cell programs targeted against other antigens and chimeric antigen receptor, or CAR-T cell programs, and which we have an option to license. For example, we may develop cellular therapies with MSK or others directed towards other viral targets such as human papilloma virus, or HPV, which is associated with cervical cancer, anal cancer, and head and neck cancer, and John Cunningham virus, which causes progressive multifocal leukoencephalopathy and is associated with a subset of solid tumors. We also intend to license or acquire additional product candidates or technologies to enhance our existing T-cell technology platform.
Our Management Team
We believe our management team has the breadth and depth of experience to execute our business model. Our management team includes:
| • | Isaac E. Ciechanover, M.D., our President and Chief Executive Officer, was Executive Director for Business Development at Celgene Corporation, or Celgene. At Celgene, he led the company’s venture capital efforts and led licensing and acquisition activities with an aggregate transaction value of more than $6.7 billion. Prior to founding Atara, Dr. Ciechanover was a Partner with Kleiner Perkins Caufield & Byers, a leading venture capital firm. |
| • | Christopher Haqq, M.D., Ph.D., our Chief Medical Officer, was Vice President for Clinical Research and Development at Cougar Biotechnology, Inc., or Cougar Biotechnology, which was acquired by Johnson & Johnson in 2009. At Cougar Biotechnology, he was the lead clinician for a pivotal prostate cancer study leading to market approval for Zytiga (abiraterone acetate). He has served as medical monitor for more than ten clinical trials and served as an attending oncology physician and director of a translational laboratory at the University of California, San Francisco. |
| • | Mitchall G. Clark, our Chief Regulatory and Quality Officer, was previously Senior Vice President of Global Regulatory Affairs at Abraxis Bioscience, Inc., or Abraxis, where he submitted and managed five INDs for oncology and cardiovascular drugs including Abraxane. |
| • | Gad Soffer, our Chief Operating Officer, previously held various roles at Celgene, including most recently Global Project Leader for Abraxane following Celgene’s acquisition of Abraxis, where he led successful regulatory submissions for pancreatic cancer and non-small cell lung cancer. |
| • | John F. McGrath, Jr., our Chief Financial Officer, was previously Executive in Residence and Operating Partner at Kleiner Perkins Caufield & Byers. Prior to that time, he served as Vice President and Chief Financial Officer for Network Equipment Technologies, Inc., a publicly traded company. |
5
Our Strategy
Our business model is to license or acquire and develop novel therapeutics for serious unmet medical needs with validated targets and established proof of concept. Based on the properties of each of these molecules, including efficacy, safety, pharmacokinetics, affinity and other characteristics, we match each program to clinical indications that we believe maximize its therapeutic potential and may result in an expedited path to market.
Our goal is to be a leader in the development and commercialization of novel therapeutics for serious unmet medical needs. We are initially focused on muscle wasting conditions, oncology and viral-associated diseases. Key components of our strategy to achieve this objective include:
| • | rapidly advance PINTA 745 in clinical development, initially for PEW; |
| • | obtain clinical proof of concept for STM 434, initially for ovarian cancer and other solid tumors; |
| • | evaluate our other molecularly targeted product candidates and advance them into the clinic as appropriate; |
| • | rapidly advance EBV-CTL in clinical development for the treatment of EBV-LPD after HCT or SOT; |
| • | develop CMV-CTL based on existing clinical proof of concept data in refractory CMV infection after HCT; |
| • | continue development of WT1-CTL and collaborate with MSK in the discovery and development of additional T-cell programs; and |
| • | leverage our relationships and experience to in-license or acquire additional product candidates for development. |
Risks Associated with Our Business
Our business is subject to numerous risks and uncertainties, including those highlighted in the section titled “Risk Factors” immediately following this prospectus summary. Some of these risks are:
| • | we have a limited operating history on which to assess our business, have generated no revenues, have incurred significant losses since our inception and anticipate that we will continue to incur losses for the foreseeable future; |
| • | we expect that we will need to raise additional financing to achieve our product candidate development, regulatory approval and commercialization goals; |
| • | we are very early in our product candidate development efforts and are heavily dependent on the regulatory approval and successful commercialization of our product candidates; |
| • | our T-cell product candidates represent new therapeutic approaches that present significant challenges; |
| • | we rely on third parties to conduct our preclinical studies and clinical trials; |
| • | we have no experience manufacturing our product candidates on a large clinical or commercial scale and are dependent on third parties to conduct such manufacturing; |
| • | our commercial success depends on attaining significant market acceptance of our product candidates, if approved, among physicians, patients, healthcare payors and major operators of dialysis and cancer centers; |
6
| • | if we are unable to obtain and maintain sufficient intellectual property protection for our product candidates, we may not be able to compete effectively; and |
| • | our future success depends in part upon our ability to retain members of our executive management team and to attract, retain and motivate other qualified personnel. |
Corporate Information
We were incorporated in August 2012 in Delaware. Our principal executive offices are located at 701 Gateway Blvd., Suite 200, South San Francisco, California 94080 and our telephone number is (650) 278-8930. Our website address is www.atarabio.com. Information contained on or accessible through our website is not a part of this prospectus and should not be relied upon in determining whether to make an investment decision.
We are an “emerging growth company” as defined in the Jumpstart Our Business Startups Act, or the JOBS Act, and therefore we may take advantage of certain exemptions from various public company reporting requirements, including not being required to have our internal control over financial reporting audited by our independent registered public accounting firm pursuant to Section 404 of the Sarbanes-Oxley Act of 2002, or the Sarbanes-Oxley Act, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and any golden parachute payments. We may take advantage of these exemptions until we are no longer an “emerging growth company.” We will remain an “emerging growth company” for up to five years. We will cease to be an “emerging growth company” upon the earliest of: (1) December 31, 2019; (2) the last day of the first fiscal year in which our annual gross revenues are $1 billion or more; (3) the date on which we have, during the previous rolling three-year period, issued more than $1 billion in nonconvertible debt securities; and (4) the date on which we are deemed to be a “large accelerated filer” as defined in the Securities Exchange Act of 1934, as amended, or the Exchange Act. We have chosen to irrevocably opt out of the extended transition periods available under the JOBS Act for complying with new or revised accounting standards.
7
The Offering
| Common stock offered by Atara |
$125,000,000 of shares |
| Option to purchase additional shares of common stock |
$18,750,000 of shares |
| Common stock to be outstanding after this offering |
shares, assuming a public offering price of $52.62 per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on June 26, 2015. |
| Use of proceeds |
We estimate that our net proceeds from this offering will be approximately $ million, or approximately $ million if the underwriters’ option to purchase additional shares of our common stock is exercised in full, after deducting underwriting discounts and commissions and estimated offering expenses. |
| We intend to use the net proceeds from this offering, along with our other capital resources, primarily (1) to complete our planned confirmatory Phase 2 clinical trial of PINTA 745, (2) to continue our initial Phase 1 clinical study of STM 434, (3) to continue the ongoing and planned studies and trials with our T-cell product candidates and (4) to continue to expand and advance our clinical and preclinical pipeline for working capital and for other general corporate purposes and to potentially acquire or license other product candidates, businesses or technologies, although we have no present commitments for any such acquisitions or licenses. See “Use of Proceeds” for additional information. |
| Risk factors |
See “Risk Factors” beginning on page 12 and the other information included in, or incorporated by reference into, this prospectus for a discussion of factors you should carefully consider before deciding to invest in our common stock. |
| Nasdaq Global Select Market symbol |
“ATRA” |
The number of shares of common stock to be outstanding after this offering is based on 24,360,247 shares of our common stock outstanding as of March 31, 2015, and excludes the following:
| • | 906,391 shares of common stock issuable upon settlement of restricted stock units, or RSUs, outstanding as of March 31, 2015; |
| • | 1,314,635 shares of common stock issuable upon the exercise of options outstanding as of March 31, 2015 with a weighted average exercise price of $19.61 per share; |
| • | 2,046,541 shares of common stock reserved for future issuance under our 2014 Equity Incentive Plan, or 2014 Plan as of March 31, 2015; |
8
| • | 432,898 shares of common stock reserved for issuance under our 2014 Employee Stock Purchase Plan, or our ESPP, as of March 31, 2015; and |
| • | any future automatic increases in the number of shares of common stock reserved for issuance under our 2014 Plan or ESPP. |
In addition, unless we specifically state otherwise, all information in this prospectus assumes no exercise of the underwriters’ option to purchase up to an additional $18,750,000 of shares of common stock from us.
9
SUMMARY CONSOLIDATED AND COMBINED FINANCIAL DATA
The following tables summarize our consolidated and combined financial data. You should read this summary consolidated and combined financial data together with the sections titled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” in our Annual Report on Form 10-K and our Quarterly Report on Form 10-Q, our consolidated and combined financial statements and related notes, each of which is incorporated by reference in this prospectus.
We have derived the summary combined statement of operations data for the years ended December 31, 2013 and 2014 from our audited consolidated and combined financial statements. We have derived the summary consolidated and combined statements of operations data for the three months ended March 31, 2014 and 2015 and our consolidated balance sheet data as of March 31, 2015 from our unaudited interim consolidated and combined financial statements. The unaudited interim consolidated and combined financial statements have been prepared on the same basis as the audited consolidated and combined financial statements and reflect, in the opinion of management, all adjustments of a normal, recurring nature that are necessary for a fair presentation of the unaudited interim consolidated and combined financial statements. Our historical results are not necessarily indicative of the results that should be expected in the future, and our interim results are not necessarily indicative of the results that should be expected for the full year or any other period.
| Year ended December 31, |
Three months ended March 31, |
|||||||||||||||
| 2013 | 2014 | 2014 | 2015 | |||||||||||||
| (In thousands, except per share information) | ||||||||||||||||
| Consolidated and Combined Statements of Income Data |
||||||||||||||||
| Operating Expenses: |
||||||||||||||||
| Research and development |
$ | 4,306 | $ | 14,380 | $ | 2,981 | $ | 5,767 | ||||||||
| Research and development costs paid to Amgen |
553 | 1,066 | ||||||||||||||
| General and administrative |
3,756 | 12,710 | 4,096 | 3,544 | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Total operating expenses |
8,615 | 28,156 | 7,077 | 9,311 | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Loss from operations |
(8,615 | ) | (28,156 | ) | (7,077 | ) | (9,311 | ) | ||||||||
| Interest and other income |
12 | 125 | 6 | 153 | ||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Loss before provision for income taxes |
(8,603 | ) | (28,031 | ) | (7,071 | ) | (9,158 | ) | ||||||||
| Provision (benefit) for income taxes |
170 | (25 | ) | (22 | ) | 2 | ||||||||||
|
|
|
|
|
|
|
|
|
|||||||||
| Net loss |
$ | (8,773 | ) | $ | (28,006 | ) | $ | (7,049 | ) | $ | (9,160 | ) | ||||
|
|
|
|
|
|
|
|
|
|||||||||
| Comprehensive loss |
$ | (8,773 | ) | $ | (28,106 | ) | $ | (7,060 | ) | $ | (9,078 | ) | ||||
|
|
|
|
|
|
|
|
|
|||||||||
| Basic and diluted net loss per common share(1) |
$ | (9.08 | ) | $ | (5.62 | ) | $ | (5.58 | ) | $ | (0.42 | ) | ||||
|
|
|
|
|
|
|
|
|
|||||||||
| (1) | Periods presented prior to our October 2014 initial public offering do not give effect to the automatic conversion of our preferred stock into common stock upon the closing of our initial public offering. |
10
| As of March 31, 2015 | ||||||||
| Actual | As Adjusted(1) | |||||||
| (In thousands) | ||||||||
| Consolidated and Combined Balance Sheet Data |
||||||||
| Cash, cash equivalents and investments |
$ | 166,696 | $ | |||||
| Working capital |
$ | 166,177 | $ | |||||
| Total assets |
$ | 169,817 | $ | |||||
| Total stockholders’ equity |
$ | 166,094 | $ | |||||
| (1) | The as adjusted column reflects the sale of shares of our common stock in this offering, at the assumed public offering price of $ per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on , 2015, after deducting underwriting discounts and commissions and estimated offering expenses. The as adjusted column does not reflect our $4.5 million obligation to MSK, incurred in June 2015 in connection with the exercise of our option to license certain T-cell product candidates from MSK. |
11
Investing in our common stock involves a high degree of risk. You should carefully consider the following risks and all of the other information included and incorporated by reference in this prospectus before investing in our common stock. While we believe that the risks and uncertainties described below are the material risks currently facing us, additional risks that we do not yet know of or that we currently think are immaterial may also arise and materially affect our business. If any of the following risks materialize, our business, financial condition and results of operations could be materially and adversely affected. In that case, the trading price of our common stock could decline, and you may lose some or all of your investment.
Risks Related to Our Financial Results and Capital Needs
We have incurred substantial losses since our inception and anticipate that we will continue to incur substantial and increasing losses for the foreseeable future.
We are a clinical-stage biopharmaceutical company. Investment in biopharmaceutical product development is highly speculative because it entails substantial upfront capital expenditures and significant risk that a product candidate will fail to prove effective, gain regulatory approval or become commercially viable. We do not have any products approved by regulatory authorities and have not generated any revenues from product sales to date, and have incurred significant research, development and other expenses related to our ongoing operations and expect to continue to incur such expenses. As a result, we have not been profitable and have incurred significant operating losses in every reporting period since our inception. For the year ended December 31, 2014 and the three months ended March 31, 2015, we reported a net loss of $28.0 million and $9.2 million, respectively, and we had an accumulated deficit of $50.0 million at March 31, 2015.
We do not expect to generate revenues for many years, if at all. We expect to continue to incur significant expenses and operating losses for the foreseeable future. We anticipate these losses to increase as we continue to research, develop and seek regulatory approvals for our product candidates and any additional product candidates we may acquire, and potentially begin to commercialize product candidates that may achieve regulatory approval. We may encounter unforeseen expenses, difficulties, complications, delays and other unknown factors that may adversely affect our business. The size of our future net losses will depend, in part, on the rate of future growth of our expenses and our ability to generate revenues. If any of our product candidates fails in clinical trials or does not gain regulatory approval, or if approved, fails to achieve market acceptance, we may never become profitable. Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods. We anticipate that our expenses will increase in the future as we continue to invest in research and development of our existing product candidates, investigate and potentially acquire new product candidates and expand our manufacturing and commercialization activities.
We have a limited operating history, which may make it difficult for you to evaluate the success of our business to date and to assess our future viability.
Our company was formed in August 2012. Our operations to date have been limited to organizing and staffing our company, acquiring product and technology rights and conducting product development activities for our product candidates. We have not yet demonstrated our ability to successfully complete any Phase 2 or Phase 3 clinical trials, obtain regulatory approval, manufacture a commercial scale product or arrange for a third party to do so on our behalf, or conduct sales and marketing activities necessary for successful commercialization for any of our product candidates. In addition, the adoptive immunotherapy technology underlying our T-cell product candidates, EBV-CTL,
12
CMV-CTL and WT1-CTL, is new and largely unproven. Any predictions about our future success, performance or viability, particularly in view of the rapidly evolving cancer immunotherapy field, may not be as accurate as they could be if we had a longer operating history or approved products on the market.
In addition, as a young business, we may encounter unforeseen expenses, difficulties, complications, delays and other known and unknown factors. We will need to transition at some point from a company with a research and development focus to a company capable of supporting commercial activities. We may not be successful in such a transition. We expect our financial condition and operating results to continue to fluctuate significantly from quarter to quarter and year to year due to a variety of factors, many of which are beyond our control. Accordingly, you should not rely upon the results of any quarterly or annual periods as indications of future operating performance.
We currently have no source of revenues. We may never generate revenues or achieve profitability.
To date, we have not generated any revenues from product sales or otherwise. Even if we are able to successfully achieve regulatory approval for our product candidates, we do not know when we will generate revenues or become profitable, if at all. Our ability to generate revenues from product sales and achieve profitability will depend on our ability to commercialize products, including any of our current product candidates, and other product candidates that we may develop, in-license or acquire in the future. Our ability to generate revenues and achieve profitability also depends on a number of additional factors, including our ability to:
| • | successfully complete development activities, including the necessary clinical trials; |
| • | complete and submit biologics license applications, or BLAs, to the FDA and obtain US regulatory approval for indications for which there is a commercial market; |
| • | complete and submit applications to, and obtain regulatory approval from, foreign regulatory authorities in Europe, Asia and other jurisdictions; |
| • | obtain coverage and adequate reimbursement from third parties, including government and private payors; |
| • | set a commercially viable price for our products; |
| • | establish and maintain supply and manufacturing relationships with reliable third parties and ensure adequate, legally compliant manufacturing of bulk drug substances and drug products to maintain that supply; |
| • | develop manufacturing and distribution processes for our novel T-cell product candidates; |
| • | obtain commercial quantities of our products at acceptable cost levels; |
| • | achieve market acceptance of our products, if any; |
| • | attract, hire and retain qualified personnel; |
| • | protect our rights in our intellectual property portfolio; |
| • | develop a commercial organization capable of sales, marketing and distribution for any products we intend to sell ourselves in the markets in which we choose to commercialize on our own; and |
| • | find suitable distribution partners to help us market, sell and distribute our approved products in other markets. |
13
Our revenues for any product candidate for which regulatory approval is obtained will be dependent, in part, upon the size of the markets in the territories for which we gain regulatory approval, the accepted price for the product, the ability to get reimbursement at any price, and whether we own the commercial rights for that territory. If the number of our addressable disease patients is not as significant as we estimate, the indication approved by regulatory authorities is narrower than we expect, or the reasonably accepted population for treatment is narrowed by competition, physician choice or treatment guidelines, we may not generate significant revenues from sales of such products, even if approved. In addition, we anticipate incurring significant costs associated with commercializing any approved product candidate. As a result, even if we generate revenues, we may not become profitable and may need to obtain additional funding to continue operations. If we fail to become profitable or are unable to sustain profitability on a continuing basis, then we may be unable to continue our operations at planned levels and may be forced to reduce our operations.
We will require substantial additional financing to achieve our goals, and a failure to obtain this necessary capital when needed could force us to delay, limit, reduce or terminate our product development or commercialization efforts.
We expect to expend substantial resources for the foreseeable future continuing the clinical development and manufacturing of PINTA 745, STM 434, EBV-CTL, CMV-CTL and WT1-CTL and the advancement and expansion of our preclinical research pipeline, including ATA 842. These expenditures will include costs associated with research and development, potentially acquiring new product candidates or technologies, conducting preclinical studies and clinical trials and potentially obtaining regulatory approvals and manufacturing products, as well as marketing and selling products approved for sale, if any. Under the terms of our license agreements with Amgen and MSK, we are obligated to make an upfront payment to MSK of $4.5 million and additional milestone payments of up to $86.0 million to Amgen and up to $33.0 million to MSK with respect to the three licensed clinical stage T-cell programs upon the achievement of certain development, regulatory approval or commercial milestones. In addition, other unanticipated costs may arise. Because the design and outcome of our planned and anticipated clinical trials is highly uncertain, we cannot reasonably estimate the actual amounts necessary to successfully complete the development and commercialization of our product candidates.
Our future capital requirements depend on many factors, including:
| • | the scope, progress, results and costs of researching and developing our other product candidates, and conducting preclinical studies and clinical trials; |
| • | the timing of, and the costs involved in, obtaining regulatory approvals for our other product candidates if clinical trials are successful; |
| • | the cost of commercialization activities for our product candidates, if any of these product candidates is approved for sale, including marketing, sales and distribution costs; |
| • | the cost of manufacturing our product candidates for clinical trials in preparation for regulatory approval and in preparation for commercialization; |
| • | our ability to establish and maintain strategic licensing or other arrangements and the financial terms of such agreements; |
| • | the costs to in-license future product candidates or technologies; |
| • | the costs involved in preparing, filing, prosecuting, maintaining, expanding, defending and enforcing patent claims, including litigation costs and the outcome of such litigation; |
| • | the timing, receipt and amount of sales of, or royalties on, our future products, if any; and |
| • | the emergence of competing technologies or other adverse market developments. |
14
Based on our current operating plan, we believe that our existing cash and cash equivalents and short-term investments, together with the net proceeds from this offering, will be sufficient to fund our projected operating requirements through the second half of 2018. As of March 31, 2015, we had cash and cash equivalents and short-term investments of $166.7 million. However, our operating plan may change as a result of many factors currently unknown to us, and we may need additional funds sooner than planned. In addition, we may seek additional capital due to favorable market conditions or strategic considerations even if we believe we have sufficient funds for our current or future operating plans. We do not have any committed external source of funds. Additional funds may not be available when we need them on terms that are acceptable to us, or at all. If adequate funds are not available to us on a timely basis, we may be required to delay, limit, reduce or terminate preclinical studies, clinical trials or other development activities for one or more of our product candidates or delay, limit, reduce or terminate our establishment of sales and marketing capabilities or other activities that may be necessary to commercialize our product candidates.
Raising additional capital may cause dilution to our existing stockholders, restrict our operations or require us to relinquish rights to our product candidates on unfavorable terms to us.
We may seek additional capital through a variety of means, including through private and public equity offerings and debt financings. To the extent that we raise additional capital through the sale of equity or convertible debt securities, your ownership interest will be diluted, and the terms may include liquidation or other preferences that adversely affect your rights as a stockholder. Debt financing, if available, may involve agreements that include covenants limiting or restricting our ability to take certain actions, such as incurring additional debt, making capital expenditures or declaring dividends. If we raise additional funds from third parties, we may have to relinquish valuable rights to our technologies or product candidates, or grant licenses on terms that are not favorable to us. If we are unable to raise additional funds through equity or debt financing when needed, we may be required to delay, limit, reduce or terminate our product development or commercialization efforts for our product candidates, or grant to others the rights to develop and market product candidates that we would otherwise prefer to develop and market ourselves.
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
We have incurred substantial losses during our history and do not expect to become profitable in the near future and we may never achieve profitability. To the extent that we continue to generate taxable losses, unused losses will carry forward to offset future taxable income, if any, until such unused losses expire. At December 31, 2014, we had federal and state net operating loss, or NOL, carryforwards of approximately $20.6 million, which, if not utilized, begin to expire in various amounts beginning in the year 2032. Under Section 382 of the Internal Revenue Code of 1986, as amended, or the Code, if over a rolling three-year period, the cumulative change in our ownership exceeds 50% (as determined under applicable Treasury regulations), our ability to utilize our US NOL carryforwards and other pre-change tax attributes (such as research tax credits) to offset future taxable income or taxes may be limited. We have experienced at least one ownership change since inception and our utilization of NOL carryforwards will therefore be subject to annual limitation. Our ability to utilize our NOL carryforwards may be further limited as a result of subsequent ownership changes, including potential changes in connection with this offering. Similar rules may apply under state tax laws. Further, other provisions of the Code may limit our ability to utilize NOLs incurred before the recapitalization to offset income or gain realized after the recapitalization, unless such income or gain is realized by the same entity that originally incurred such NOLs. In addition, at the state level, there may be periods during which the use of NOLs is suspended or otherwise limited. Such limitations could result in the expiration of our carryforwards before they can be utilized and, if we are profitable, our future cash flows could be adversely affected due to our increased tax liability.
15
Risks Related to the Development of Our Product Candidates
We are very early in our development efforts and have only five product candidates in clinical development. All of our other product candidates are still in preclinical development. If we or our collaborators are unable to successfully develop and commercialize product candidates or experience significant delays in doing so, our business will be materially harmed.
We are very early in our development efforts. We have five product candidates, PINTA 745, STM 434, EBV-CTL, CMV-CTL and WT1-CTL, in clinical development. All of our other product candidates are currently in preclinical development. We have invested substantially all of our efforts and financial resources in identifying and developing potential product candidates and conducting preclinical studies, clinical trials and manufacturing activities. Our ability to generate revenues, which we do not expect will occur for many years, if ever, will depend heavily on the successful development and eventual commercialization of our product candidates. The success of our product candidates will depend on several factors, including the following:
| • | completion of preclinical studies and clinical trials with positive results; |
| • | receipt of regulatory approvals from applicable authorities; |
| • | obtaining and maintaining patent and trade secret protection and regulatory exclusivity for our product candidates; |
| • | making arrangements with third-party manufacturers for, or establishing, commercial manufacturing capabilities; |
| • | develop manufacturing and distribution processes for our novel T-cell product candidates; |
| • | manufacturing products at an acceptable cost; |
| • | launching commercial sales of our product candidates, if and when approved, whether alone or in collaboration with others; |
| • | acceptance of the product candidates, if and when approved, by patients, the medical community and third-party payors; |
| • | effectively competing with other therapies; |
| • | obtaining and maintaining coverage and adequate reimbursement by third-party payors, including government payors, for our product candidates; |
| • | protecting our rights in our intellectual property portfolio; |
| • | maintaining a continued acceptable safety profile of the products following approval; and |
| • | maintaining and growing an organization of scientists and business people who can develop and commercialize our products and technology. |
If we do not achieve one or more of these factors in a timely manner or at all, we could experience significant delays or an inability to successfully develop and commercialize our product candidates, which would materially harm our business.
Our future success is dependent on the regulatory approval of our product candidates.
We do not have any products that have gained regulatory approval. Currently, our only clinical-stage product candidates are PINTA 745, EBV-CTL and CMV-CTL, which are in Phase 2 clinical trials, and STM 434 and WT1-CTL, which are in Phase 1 clinical studies. Our business is substantially dependent on our ability to obtain regulatory approval for, and, if approved, to successfully commercialize our product candidates in a timely manner. We cannot commercialize product candidates in the United States without first obtaining regulatory approval for the product from the FDA;
16
similarly, we cannot commercialize product candidates outside of the United States without obtaining regulatory approval from comparable foreign regulatory authorities. Before obtaining regulatory approvals for the commercial sale of any product candidate for a target indication, we must demonstrate with substantial evidence gathered in preclinical and clinical studies, generally including two well-controlled Phase 3 trials, that the product candidate is safe and effective for use for that target indication and that the manufacturing facilities, processes and controls are adequate with respect to such product candidate.
The time required to obtain approval by the FDA and comparable foreign regulatory authorities is unpredictable but typically takes many years following the commencement of preclinical studies and clinical trials and depends upon numerous factors, including the substantial discretion of the regulatory authorities. In addition, approval policies, regulations, or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions. We have not obtained regulatory approval for any product candidate and it is possible that none of our existing product candidates or any future product candidates will ever obtain regulatory approval.
Our product candidates could fail to receive regulatory approval from the FDA or a comparable foreign regulatory authority for many reasons, including:
| • | disagreement with the design or implementation of our clinical trials; |
| • | failure to demonstrate that a product candidate is safe and effective for its proposed indication; |
| • | failure of clinical trials to meet the level of statistical significance required for approval; |
| • | failure to demonstrate that a product candidate’s clinical and other benefits outweigh its safety risks; |
| • | disagreement with our interpretation of data from preclinical studies or clinical trials; |
| • | the insufficiency of data collected from clinical trials of our product candidates to support the submission and filing of a BLA or other submission or to obtain regulatory approval; |
| • | failure to obtain approval of the manufacturing processes or facilities of third-party manufacturers with whom we contract for clinical and commercial supplies; or |
| • | changes in the approval policies or regulations that render our preclinical and clinical data insufficient for approval. |
The FDA or a comparable foreign regulatory authority may require more information, including additional preclinical or clinical data to support approval, which may delay or prevent approval and our commercialization plans, or we may decide to abandon the development program. If we were to obtain approval, regulatory authorities may approve any of our product candidates for fewer or more limited indications than we request (including failing to approve the most commercially promising indications), may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve a product candidate with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that product candidate.
Even if a product candidate were to successfully obtain approval from the FDA and comparable foreign regulatory authorities, any approval might contain significant limitations related to use restrictions for specified age groups, warnings, precautions or contraindications, or may be subject to burdensome post-approval study or risk management requirements. If we are unable to obtain regulatory approval for one of our product candidates in one or more jurisdictions, or any approval contains significant limitations, we may not be able to obtain sufficient funding to continue the development of that product or generate revenues attributable to that product candidate. Also, any regulatory approval of our current or future product candidates, once obtained, may be withdrawn.
17
Our T-cell product candidates, EBV-CTL, CMV-CTL and WT1-CTL, represent new therapeutic approaches that present significant challenges.
Our future success is dependent in part on the successful development of T-cell immunotherapies in general and our EBV-CTL, CMV-CTL and WT1-CTL product candidates in particular. Because these programs represent a new approach to immunotherapy for the treatment of cancer and other diseases, developing and commercializing our product candidates subject us to a number of challenges, including:
| • | obtaining regulatory approval from the FDA and other regulatory authorities, which have very limited experience with the commercial development of T-cell therapies; |
| • | developing and deploying consistent and reliable processes for procuring blood from consenting third-party donors, isolating T-cells from the blood of such donors, activating the isolated T-cells against a specific antigen, characterizing and storing the resulting activated T-cells for future therapeutic use, selecting and delivering an appropriate partially HLA matched cell line from among the available T-cell lines, and finally infusing these activated T-cells into patients; |
| • | utilizing these product candidates in combination with other therapies, which may increase the risk of adverse side effects; |
| • | educating medical personnel regarding the potential side effect profile of each of our product candidates; |
| • | developing processes for the safe administration of these products, including long-term follow-up for all patients who receive these product candidates; |
| • | sourcing clinical and, if approved, commercial supplies for the materials used to manufacture and process these product candidates; |
| • | developing a manufacturing process and distribution network with a cost of goods that allows for an attractive return on investment; |
| • | establishing sales and marketing capabilities after obtaining any regulatory approval to gain market acceptance, and obtaining adequate coverage, reimbursement and pricing by third-party payors and government authorities; and |
| • | developing therapies for types of diseases beyond those initially addressed by our current product candidates. |
We cannot be sure that the manufacturing processes used in connection with our T-cell product candidates, EBV-CTL, CMV-CTL and WT1-CTL, will yield satisfactory products that are safe and effective, scalable or profitable.
Moreover, public perception of therapy safety issues, including adoption of new therapeutics or novel approaches to treatment, may adversely influence the willingness of subjects to participate in clinical trials, or if approved, of physicians to subscribe to the novel treatment mechanics. Physicians, hospitals and third-party payors often are slow to adopt new products, technologies and treatment practices that require additional upfront costs and training. Physicians may not be willing to undergo training to adopt this novel therapy, may decide the therapy is too complex to adopt without appropriate training and may choose not to administer the therapy. Based on these and other factors, hospitals and payors may decide that the benefits of this new therapy do not or will not outweigh its costs.
18
The results of preclinical testing or earlier clinical studies are not necessarily predictive of future results. Our existing product candidates in clinical studies or trials, and any other product candidate we advance into clinical studies or trials, may not have favorable results in later clinical studies or trials or receive regulatory approval.
Success in preclinical studies and early clinical trials does not ensure that later clinical trials will generate adequate data to demonstrate the efficacy and safety of an investigational drug. A number of companies in the pharmaceutical and biotechnology industries, including those with greater resources and experience than us, have suffered significant setbacks in clinical trials, even after seeing promising results in earlier preclinical studies or clinical studies or trials. Despite the results reported in earlier preclinical studies or clinical studies or trials for our product candidates, we do not know whether the clinical trials we may conduct will demonstrate adequate efficacy and safety to result in regulatory approval to market PINTA 745, STM 434, EBV-CTL, CMV-CTL or WT1-CTL or any of our other product candidates in any particular jurisdiction. For example, our EBV-CTL, CMV-CTL and WT1-CTL product candidates have only been evaluated in single-center studies under investigator-sponsored INDs held by MSK, and the findings may not be reproducible in multi-center studies conducted under commercially-sponsored INDs. In addition, the Phase 2 clinical trials with EBV-CTL enrolled a heterogeneous group of patients with a variety of EBV-associated malignancies, including but not limited to EBV-LPD after HCT and EBV-LPD after SOT. These Phase 2 studies were not prospectively designed to evaluate the efficacy of EBV-CTL in the treatment of a single disease state for which we may later seek approval. Efficacy data from prospectively designed studies may differ significantly from those obtained from retrospective subgroup analyses. If later-stage clinical trials do not produce favorable results, our ability to achieve regulatory approval for any of our product candidates may be adversely impacted. Even if we believe that we have adequate data to support an application for regulatory approval to market any of our product candidates, the FDA or other regulatory authorities may not agree and may require that we conduct additional clinical trials.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through preclinical and clinical studies and early clinical trials.
We may experience delays in our ongoing or future clinical studies or trials and we do not know whether planned clinical studies or trials will begin or enroll subjects on time, will need to be redesigned or will be completed on schedule, if at all. There can be no assurance that the FDA will not put clinical studies or trials of any of our product candidates on clinical hold in the future. Clinical studies or trials may be delayed, suspended or prematurely terminated for a variety of reasons, such as:
| • | delay or failure in reaching agreement with the FDA or a comparable foreign regulatory authority on a study or trial design that we are able to execute; |
| • | delay or failure in obtaining authorization to commence a study or trial or inability to comply with conditions imposed by a regulatory authority regarding the scope or design of a study or trial; |
| • | delay or failure in reaching agreement on acceptable terms with prospective contract research organizations, or CROs, and clinical study or trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and study or trial sites; |
| • | delay or failure in obtaining institutional review board, or IRB, approval or the approval of other reviewing entities, including comparable foreign regulatory authorities, to conduct a clinical study or trial at each site; |
19
| • | withdrawal of clinical study or trial sites from our clinical studies or trials or the ineligibility of a site to participate in our clinical studies or trials; |
| • | delay or failure in recruiting and enrolling suitable subjects to participate in a study or trial; |
| • | delay or failure in subjects completing a study or trial or returning for post-treatment follow-up; |
| • | clinical sites and investigators deviating from trial protocol, failing to conduct the study or trial in accordance with regulatory requirements, or dropping out of a study or trial; |
| • | inability to identify and maintain a sufficient number of study or trial sites, many of which may already be engaged in other clinical study or trial programs, including some that may be for the same indication; |
| • | failure of our third-party clinical study or trial managers to satisfy their contractual duties, meet expected deadlines or return trustworthy data; |
| • | delay or failure in adding new study or trial sites; |
| • | interim results or data that are ambiguous or negative or are inconsistent with earlier results or data; |
| • | feedback from the FDA, the IRB, data safety monitoring boards or a comparable foreign regulatory authority, or results from earlier stage or concurrent preclinical and clinical studies, that might require modification to the protocol for a study or trial; |
| • | a decision by the FDA, the IRB, a comparable foreign regulatory authority, or us, or a recommendation by a data safety monitoring board or comparable foreign regulatory authority, to suspend or terminate clinical studies or trials at any time for safety issues or for any other reason; |
| • | unacceptable risk-benefit profile, unforeseen safety issues or adverse side effects; |
| • | failure to demonstrate a benefit from using a drug; |
| • | difficulties in manufacturing or obtaining from third parties sufficient quantities of a product candidate for use in studies or trials; |
| • | lack of adequate funding to continue a study or trial, including the incurrence of unforeseen costs due to enrollment delays, requirements to conduct additional studies or increased expenses associated with the services of our CROs and other third parties; or |
| • | changes in governmental regulations or administrative actions or lack of adequate funding to continue a clinical study or trial. |
Patient enrollment, a significant factor in the timing of clinical studies or trials, is affected by many factors including the size and nature of the patient population, the severity of the disease under investigation, the proximity of subjects to clinical sites, the patient referral practices of physicians, the eligibility criteria for the study or trial, the design of the clinical study or trial, ability to obtain and maintain patient consents, risk that enrolled subjects will drop out before completion, competing clinical studies or trials and clinicians’ and patients’ perceptions as to the potential advantages and risks of the drug being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. We may not be able to initiate or continue to support clinical trials of PINTA 745, EBV-CTL or CMV-CTL or clinical studies for STM 434 or WT1-CTL or any future product candidates if we are unable to locate and enroll a sufficient number of eligible participants in these studies or trials as required by the FDA or other regulatory authorities. Even if we are able to enroll a sufficient number of patients in our clinical studies or trials, if the pace of enrollment is slower than we expect, the development costs for our product candidates may increase and the completion of our studies may be delayed or our studies or trials could become too expensive to
20
complete. We rely on CROs, other vendors and clinical study or trial sites to ensure the proper and timely conduct of our clinical studies and trials, and while we have agreements governing their committed activities, we have limited influence over their actual performance.
If we experience delays in the completion or termination of any clinical study or trial of our product candidates, the commercial prospects of such product candidate will be harmed, and our ability to generate product revenues from such product candidate will be delayed. In addition, any delays in completing our clinical studies or trials will increase our costs, slow down our product candidate development and approval process and jeopardize our ability to commence product sales and generate revenues. Any delays in completing our clinical studies or trials for the product candidates we have licensed from Amgen or MSK may also decrease the period of commercial exclusivity under our corresponding product candidate license from Amgen or MSK. In addition, many of the factors that could cause a delay in the commencement or completion of clinical studies or trials may also ultimately lead to the denial of regulatory approval of our product candidates.
Our product candidates, the methods used to deliver them or their dosage levels may cause undesirable side effects or have other properties that could delay or prevent their regulatory approval, limit the commercial profile of an approved label or result in significant negative consequences following any regulatory approval.
Undesirable side effects caused by our product candidates, their delivery methods or dosage levels could cause us or regulatory authorities to interrupt, delay or halt clinical trials and could result in a more restrictive label or the delay or denial of regulatory approval by the FDA or other comparable foreign regulatory authority. As a result of safety or toxicity issues that we may experience in our clinical studies or trials in the future, we may not receive approval to market any product candidates, which could prevent us from ever generating revenues or achieving profitability. Results of our studies or trials could reveal an unacceptably high severity and prevalence of side effects. In such an event, our studies or trials could be suspended or terminated and the FDA or comparable foreign regulatory authorities could order us to cease further development of or deny approval of our product candidates for any or all targeted indications. The drug-related side effects could affect patient recruitment or the ability of enrolled subjects to complete the trial or result in potential product liability claims. Any of these occurrences may have a material adverse effect on our business, results of operations, financial condition, cash flows and future prospects.
Additionally, if any of our product candidates receives regulatory approval, and we or others later identify undesirable side effects caused by such product, a number of potentially significant negative consequences could result, including that:
| • | we may be forced to suspend marketing of such product; |
| • | regulatory authorities may withdraw their approvals of such product; |
| • | regulatory authorities may require additional warnings on the label that could diminish the usage or otherwise limit the commercial success of such products; |
| • | we may be required to conduct post-market studies; |
| • | we may be required to change the way the product is administered; |
| • | we could be sued and held liable for harm caused to subjects or patients; and |
| • | our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the particular product candidate, if approved.
21
We may not be able to obtain orphan drug exclusivity for our product candidates.
Regulatory authorities in some jurisdictions, including the United States and Europe, may designate drugs for relatively small patient populations as orphan drugs. Under the Orphan Drug Act, the FDA may designate a product as an orphan drug if it is a drug intended to treat a rare disease or condition, which is generally defined as a patient population of fewer than 200,000 individuals annually in the United States. If our Phase 1 clinical study of STM 434 is successful, we intend to apply for orphan drug status for STM 434 for ovarian cancer. In addition, we may seek orphan drug status for EBV-CTL in rituximab refractory EBV-LPD after HCT, for EBV-CTL in EBV-LPD after SOT, for CMV-CTL in refractory CMV infection after HCT and for WT1-CTL in AML and multiple myeloma.
Generally, if a product with an orphan drug designation subsequently receives the first regulatory approval for the indication for which it has such designation, the product is entitled to a period of marketing exclusivity, which precludes the European Medicines Agency, or EMA, or the FDA from approving another marketing application for the same drug for that time period. The applicable period is seven years in the United States and ten years in Europe. The European exclusivity period can be reduced to six years if a drug no longer meets the criteria for orphan drug designation or if the drug is sufficiently profitable so that market exclusivity is no longer justified. Orphan drug exclusivity may be lost if the FDA or EMA determines that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantity of the drug to meet the needs of patients with the rare disease or condition.
Even if we obtain orphan drug exclusivity for a product, that exclusivity may not effectively protect the product from competition because different drugs can be approved for the same condition. Even after an orphan drug is approved, the FDA can subsequently approve a new drug for the same condition if the FDA concludes that the later drug is clinically superior in that it is shown to be safer, more effective or makes a major contribution to patient care.
Failure to obtain regulatory approval in international jurisdictions would prevent our product candidates from being marketed abroad.
In addition to regulations in the United States, to market and sell our products in the European Union, many Asian countries and other jurisdictions, we must obtain separate regulatory approvals and comply with numerous and varying regulatory requirements. We have had no significant interactions with foreign regulatory authorities to date. The approval procedure varies among countries and can involve additional testing. The time required to obtain approval may differ substantially from that required to obtain FDA approval. The regulatory approval process outside the United States generally includes all of the risks associated with obtaining FDA approval. Clinical trials accepted in one country may not be accepted by regulatory authorities in other countries. In addition, many countries outside the United States require that a product be approved for reimbursement before it can be approved for sale in that country. We may not be able to obtain approvals from regulatory authorities outside the United States on a timely basis, if at all. Approval by the FDA does not ensure approval by regulatory authorities in other countries or jurisdictions, and approval by one regulatory authority outside the United States does not ensure approval by regulatory authorities in other countries or jurisdictions or by the FDA. We may not be able to file for regulatory approvals and may not receive necessary approvals to commercialize our products in any market. If we are unable to obtain approval of any of our product candidates by regulatory authorities in the European Union, Asia or elsewhere, the commercial prospects of that product candidate may be significantly diminished, our business prospects could decline and this could materially adversely affect our business, results of operations and financial condition.
22
Even if our product candidates receive regulatory approval, they may still face future development and regulatory difficulties.
Even if we obtain regulatory approval for a product candidate, it would be subject to ongoing requirements by the FDA and comparable foreign regulatory authorities governing the manufacture, quality control, further development, labeling, packaging, storage, distribution, adverse event reporting, safety surveillance, import, export, advertising, promotion, recordkeeping and reporting of safety and other post-market information. These requirements include submissions of safety and other post-marketing information and reports, registration, as well as continued compliance by our contract manufacturing organizations, or CMOs, and CROs for any post-approval clinical trials that we conduct. For example, if labeling is ultimately approved for PINTA 745, it will likely include restrictions on use due to the specific patient population and manner of use in which the product candidate was evaluated and the safety and efficacy data obtained in those evaluations. In addition, PINTA 745 may be required to include a boxed warning, or “black box,” regarding PINTA 745 being teratogenic, or causing fetal or embryotic malformations, in animal studies. The safety profile of any product will continue to be closely monitored by the FDA and comparable foreign regulatory authorities after approval. If the FDA or comparable foreign regulatory authorities become aware of new safety information after approval of any of our product candidates, they may require labeling changes or establishment of a risk evaluation and mitigation strategy, impose significant restrictions on a product’s indicated uses or marketing or impose ongoing requirements for potentially costly post-approval studies or post-market surveillance.
In addition, manufacturers of drug products and their facilities are subject to continual review and periodic inspections by the FDA and other regulatory authorities for compliance with current good manufacturing practices, or cGMP, current Good Clinical Practices, or GCP, good tissue practices, or GTPs, and other regulations. If we or a regulatory agency discover previously unknown problems with a product, such as adverse events of unanticipated severity or frequency, or problems with the facility where the product is manufactured, a regulatory agency may impose restrictions on that product, the manufacturing facility or us, including requiring recall or withdrawal of the product from the market or suspension of manufacturing. If we, our product candidates or the manufacturing facilities for our product candidates fail to comply with applicable regulatory requirements, a regulatory agency may:
| • | issue warning letters or untitled letters; |
| • | mandate modifications to promotional materials or require us to provide corrective information to healthcare practitioners; |
| • | require us to enter into a consent decree, which can include imposition of various fines, reimbursements for inspection costs, required due dates for specific actions and penalties for noncompliance; |
| • | seek an injunction or impose civil or criminal penalties or monetary fines; |
| • | suspend or withdraw regulatory approval; |
| • | suspend any ongoing clinical studies; |
| • | refuse to approve pending applications or supplements to applications filed by us; |
| • | suspend or impose restrictions on operations, including costly new manufacturing requirements; or |
| • | seize or detain products, refuse to permit the import or export of products, or require us to initiate a product recall. |
The occurrence of any event or penalty described above may inhibit our ability to commercialize our products and generate revenues.
23
Advertising and promotion of any product candidate that obtains approval in the United States will be heavily scrutinized by the FDA, the Department of Justice, or the DOJ, the Office of Inspector General of the Department of Health and Human Services, or HHS, state attorneys general, members of Congress and the public. Additionally, advertising and promotion of any product candidate that obtains approval outside of the United States will be heavily scrutinized by comparable foreign regulatory authorities. For example, in the event PINTA 745 obtains regulatory approval, we believe these authorities will closely monitor the use of this product candidate to determine whether it is being used impermissibly as a muscle-builder by athletes and others. Violations, including actual or alleged promotion of our products for unapproved or off-label uses, are subject to enforcement letters, inquiries and investigations, and civil and criminal sanctions by the FDA. Any actual or alleged failure to comply with labeling and promotion requirements may have a negative impact on our business.
In the United States, engaging in impermissible promotion of our products for off-label uses can also subject us to false claims litigation under federal and state statutes, which can lead to civil and criminal penalties and fines and agreements that would materially restrict the manner in which we promote or distribute our drug products. These false claims statutes include the federal False Claims Act, which allows any individual to bring a lawsuit against a pharmaceutical company on behalf of the federal government alleging submission of false or fraudulent claims, or causing to present such false or fraudulent claims, for payment by a federal program such as Medicare or Medicaid. If the government prevails in the lawsuit, the individual will share in any fines or settlement funds. Since 2004, these False Claims Act lawsuits against pharmaceutical companies have increased significantly in volume and breadth, leading to several substantial civil and criminal settlements based on certain sales practices promoting off-label drug uses. This growth in litigation has increased the risk that a pharmaceutical company will have to defend a false claim action, pay settlement fines or restitution, agree to comply with burdensome reporting and compliance obligations, and be excluded from the Medicare, Medicaid and other federal and state healthcare programs. If we do not lawfully promote our approved products, we may become subject to such litigation and, if we are not successful in defending against such actions, those actions could compromise our ability to become profitable or adversely affect our ability to operate our business.
We are subject to a multitude of manufacturing risks, any of which could substantially increase our costs and limit supply of our product candidates.
Concurrent with the license of our existing product candidates, we acquired manufacturing process know-how and certain intermediates, as well as certain supplies intended for clinical use, from Amgen and MSK. We are in the process of planning for the manufacture of additional drug substance and drug product for our preclinical and clinical studies using the know-how and supplies we received from Amgen and MSK. Our CMOs will need to conduct significant development work to prepare each of our product candidates for studies, trials and commercial readiness.
The processes by which our product candidates are manufactured were initially developed by Amgen and MSK for clinical purposes. We intend to improve these existing processes for more advanced clinical trials or commercialization. Developing commercially viable manufacturing processes is a difficult and uncertain task, and there are risks associated with scaling to the level required for advanced clinical trials or commercialization, including cost overruns, potential problems with process scale-out, process reproducibility, stability issues, lost consistency and timely availability of reagents or raw materials. The manufacturing facilities in which our product candidates will be made could be adversely affected by earthquakes and other natural disasters, equipment failures, labor shortages, power failures, and numerous other factors.
24
Additionally, the process of manufacturing biologics and cellular therapies is complex, highly regulated and subject to several risks, including but not limited to:
| • | the process of manufacturing biologics and cellular therapies is extremely susceptible to product loss due to contamination, equipment failure or improper installation or operation of equipment, or vendor or operator error. Even minor deviations from normal manufacturing processes for any of our product candidates could result in reduced production yields, product defects, and other supply disruptions. Product defects can also occur unexpectedly. For example, in April 2014, we encountered a small number of cracked vials in certain STM 434 drug product lots. If microbial, viral, or other contaminations are discovered in our product candidates or in the manufacturing facilities in which our product candidates are made, such manufacturing facilities may need to be closed for an extended period of time to allow us to investigate and remedy the contamination; and |
| • | because EBV-CTL, CMV-CTL and WT1-CTL are manufactured from the blood of third-party donors, the process of developing commercializable products may be particularly challenging, even if they otherwise prove to be safe and effective. The manufacture of these product candidates involves complex processes. Some of these processes require specialized equipment and highly skilled and trained personnel. The process of manufacturing these product candidates will be susceptible to additional risks, given the need to maintain aseptic conditions throughout the manufacturing process. Contamination in the donor material or ingress of microbiological material at any point in the process may result in contaminated and unusable product. Furthermore, the product ultimately consists of many individual cell lines, each with a different HLA profile. As a result, the selection and distribution of the appropriate cell line for therapeutic use in a patient will require close coordination between clinical and manufacturing personnel. |
Any adverse developments affecting manufacturing operations for our product candidates may result in shipment delays, inventory shortages, lot failures, withdrawals or recalls or other interruptions in the supply of our drug substance and drug product. We may also have to write off inventory, incur other charges and expenses for supply of drug product that fails to meet specifications, undertake costly remediation efforts, or seek more costly manufacturing alternatives. Inability to meet the demand for our products could damage our reputation and the reputation of our products among physicians, healthcare payors, patients or the medical community, including major operators of dialysis and cancer clinics, which could adversely affect our ability to operate our business and our results of operations.
We may not successfully identify, acquire, develop or commercialize new potential product candidates.
Part of our business strategy is to expand our product candidate pipeline by identifying and validating new product candidates, which we may develop ourselves, in-license or otherwise acquire from others. In addition, in the event that our existing product candidates do not receive regulatory approval or are not successfully commercialized, then the success of our business will depend on our ability to expand our product pipeline through in-licensing or other acquisitions. We may be unable to identify relevant product candidates. If we do identify such product candidates, we may be unable to reach acceptable terms with any third party from which we desire to in-license or acquire them.
We may not realize the benefits of strategic alliances that we may form in the future.
We may form strategic alliances, create joint ventures or collaborations or enter into licensing arrangements with third parties that we believe will complement or augment our existing business. These relationships, or those like them, may require us to incur nonrecurring and other charges, increase our near- and long-term expenditures, issue securities that dilute our existing stockholders or
25
disrupt our management and business. In addition, we face significant competition in seeking appropriate strategic alliances and the negotiation process is time-consuming and complex. Moreover, we may not be successful in our efforts to establish a strategic alliance or other alternative arrangements for any future product candidates and programs because our research and development pipeline may be insufficient, our product candidates and programs may be deemed to be at too early a stage of development for collaborative effort and third parties may not view our product candidates and programs as having the requisite potential to demonstrate safety and efficacy. If we license products or acquire businesses, we may not be able to realize the benefit of such transactions if we are unable to successfully integrate them with our existing operations and company culture. We cannot be certain that, following a strategic transaction or license, we will achieve the revenues or specific net income that justifies such transaction. Any delays in entering into new strategic alliances agreements related to our product candidates could also delay the development and commercialization of our product candidates and reduce their competitiveness even if they reach the market.
Risks Related to Our Dependence on Third Parties
We rely on third parties to conduct our preclinical and clinical studies and clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, or if we lose any of our CROs, we may not be able to obtain regulatory approval for or commercialize our product candidates on a timely basis, if at all.
We have relied upon and plan to continue to rely upon third-party CROs and contractors to monitor and manage data for our ongoing preclinical and clinical programs. For example, our collaborating investigators at MSK manage the conduct of the ongoing clinical studies and trials of EBV-CTL, CMV-CTL and WT1-CTL as well as perform the analysis, publication and presentation of data and results related to these programs. We are also relying on CROs to perform similar services for our ongoing clinical trial of PINTA 745 and clinical study of STM 434. We have also relied on studies previously conducted by Amgen and MSK. We rely on these parties for the execution of our preclinical and clinical trials, and we control only some aspects of their activities. Nevertheless, we are responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol and legal, regulatory and scientific standards, and our reliance on the CROs does not relieve us of our regulatory responsibilities. We also rely on third parties to assist in conducting our preclinical studies in accordance with Good Laboratory Practices, or GLP, and the Animal Welfare Act requirements. We and our CROs are required to comply with federal regulations, GCP, which are international standards meant to protect the rights and health of patients that are enforced by the FDA, the Competent Authorities of the Member States of the European Economic Area and comparable foreign regulatory authorities for all of our products in clinical development, and GTP, which are standards designed to ensure that cell and tissue based products are manufactured in a manner designed to prevent the introduction, transmission and spread of communicable diseases. Regulatory authorities enforce GCP and GTP through periodic inspections of trial sponsors, principal investigators and trial sites. If we or any of our CROs fail to comply with applicable GCP or GTP, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our regulatory applications. We cannot assure you that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials comply with GCP or GTP requirements. In addition, our clinical trials must be conducted with product produced under cGMP requirements. We are also required to register ongoing clinical trials and post the results of completed clinical trials on a government-sponsored database, clinicaltrials.gov, within a specified timeframe. Failure to comply with these regulations may require us to repeat preclinical and clinical trials, which would delay the regulatory approval process and result in adverse publicity.
26
Our CROs are not our employees, and except for remedies available to us under our agreements with such CROs, we cannot control whether or not they devote sufficient time and resources, including experienced staff, to our ongoing clinical, nonclinical and preclinical programs. They may also have relationships with other entities, some of which may be our competitors. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to obtain regulatory approval for or successfully commercialize our product candidates. For example, there was an error in the randomization of patients and inventory distribution to our clinical sites for our Phase 2 clinical trial for PINTA 745, resulting in the unblinding of the initial six patients and a restart of the trial. CRO or contractor errors could cause our results of operations and the commercial prospects for our product candidates to be harmed, our costs to increase and our ability to generate revenues to be delayed.
Our internal capacity for clinical trial execution and management is limited and therefore we have relied on third parties. Outsourcing these functions involves risk that third parties may not perform to our standards, may not produce results or data in a timely manner or may fail to perform at all. For example, in July 2014, we became aware of a draft report for a preclinical study conducted with STM 217, a compound similar to STM 434 that we also licensed from Amgen. Results from this study led to the amendment of our planned clinical trial for STM 434. Other data from studies previously conducted by Amgen or MSK may emerge in the future. In addition, the use of third-party service providers requires us to disclose our proprietary information to these parties, which could increase the risk that this information will be misappropriated. We currently have a small number of employees, which limits the internal resources we have available to identify and monitor our third-party providers. To the extent we are unable to identify and successfully manage the performance of third-party service providers in the future, our business may be adversely affected. Though we carefully manage our relationships with our CROs, there can be no assurance that we will not encounter challenges or delays in the future or that these delays or challenges will not have a material adverse impact on our business, financial condition and prospects.
Our CROs have the right to terminate their agreements with us in the event of an uncured material breach. In addition, some of our CROs have an ability to terminate their respective agreements with us if it can be reasonably demonstrated that the safety of the subjects participating in our clinical trials warrants such termination, if we make a general assignment for the benefit of our creditors or if we are liquidated. Identifying, qualifying and managing performance of third-party service providers can be difficult, time consuming and cause delays in our development programs. In addition, there is a natural transition period when a new CRO commences work and the new CRO may not provide the same type or level of services as the original provider. If any of our relationships with our third-party CROs terminate, we may not be able to enter into arrangements with alternative CROs or to do so on commercially reasonable terms.
We have no experience manufacturing our product candidates on a clinical or commercial scale and have no manufacturing facility. We are dependent on third parties for the manufacturing of our product candidates and our supply chain, and if we experience problems with any of these third parties, the manufacturing of our product candidates could be delayed.
We do not own or operate facilities for the manufacturing of our product candidates. We currently have no commitments to build our own clinical or commercial scale manufacturing capabilities. We currently rely on single source CMOs for the production of the product candidates we have licensed from Amgen and on single source suppliers of some of the materials incorporated in these product candidates. In the case of EBV-CTL, CMV-CTL and WT1-CTL, we rely on MSK for the production of these product candidates and acquisition of the materials incorporated in these product candidates. To
27
meet our projected needs for clinical supplies to support our activities through regulatory approval and commercial manufacturing of PINTA 745, STM 434 and the other product candidates we have licensed from Amgen, the CMOs with whom we currently work will need to increase the scale of production and demonstrate comparability of the material produced by these CMOs to the material that was previously produced by Amgen. To meet our projected needs for clinical and commercial materials to support our activities through regulatory approval and commercial manufacturing of EBV-CTL, CMV-CTL and WT1-CTL, we will need to transition the manufacturing of such materials to a CMO or our own facility, and such CMOs or we will need to increase the scale of production and demonstrate comparability of the material produced at these facilities to the material that was previously produced by MSK. We need to identify CMOs for the production of EBV-CTL, CMV-CTL and WT1-CTL and may need to identify additional CMOs for continued production of supply for all of our product candidates. In addition, given the manufacturing process for our T-cell product candidates, the number of CMOs who possess the requisite skill and capability to manufacture our T-cell product candidates is limited. We have not yet identified alternate suppliers in the event the current CMOs that we utilize are unable to scale production, or if we otherwise experience any problems with them. Manufacturing biologic drugs is complicated and tightly regulated by the FDA and comparable regulatory authorities around the world, and although alternative third-party suppliers with the necessary manufacturing and regulatory expertise and facilities exist, it could be expensive and take a significant amount of time to arrange for alternative suppliers, transfer manufacturing procedures to these alternative suppliers, and demonstrate comparability of material produced by such new suppliers. New manufacturers of any product would be required to qualify under applicable regulatory requirements. These manufacturers may not be able to manufacture our compounds at costs, or in quantities, or in a timely manner necessary to complete development of our product candidates or make commercially successful products. If we are unable to arrange for alternative third-party manufacturing sources, or to do so on commercially reasonable terms or in a timely manner, we may not be able to complete development of our product candidates, or market or distribute them. In addition, should the FDA not agree with our physical quality specifications and comparability assessments for these materials, further clinical development of our product candidate would be substantially delayed and we would incur substantial additional expenses.
Reliance on third-party manufacturers entails risks to which we would not be subject if we manufactured product candidates ourselves, including reliance on the third party for regulatory compliance and quality assurance, the possibility of breach of the manufacturing agreement by the third party because of factors beyond our control, including a failure to synthesize and manufacture our product candidates or any products we may eventually commercialize in accordance with our specifications, misappropriation of our proprietary information, including our trade secrets and know-how, and the possibility of termination or nonrenewal of the agreement by the third party, based on its own business priorities, at a time that is costly or damaging to us. In addition, the FDA and other regulatory authorities require that our product candidates and any products that we may eventually commercialize be manufactured according to cGMP and similar foreign standards. These requirements include, among other things, quality control, quality assurance and the maintenance of records and documentation. The FDA or similar foreign regulatory agencies may also implement new standards at any time, or change their interpretations and enforcement of existing standards for manufacture, packaging or testing of products. We have little control over our manufacturers’ compliance with these regulations and standards. Any failure by our third-party manufacturers to comply with cGMP or failure to scale up manufacturing processes, including any failure to deliver sufficient quantities of product candidates in a timely manner, could lead to a delay in, or failure to obtain, regulatory approval of any of our product candidates. In addition, such failure could be the basis for the FDA to issue a warning letter, withdraw approvals for product candidates previously granted to us, or take other regulatory or legal action, including recall or seizure of outside supplies of the product candidate, total or partial suspension of production, suspension of ongoing clinical trials, refusal to approve pending applications or supplemental applications, detention or product, refusal to permit the import or export of products, injunction or imposing civil and criminal penalties.
28
Any significant disruption in our supplier relationships could harm our business. Any significant delay in the supply of a product candidate or its key materials for an ongoing clinical study could considerably delay completion of our clinical studies, product testing and potential regulatory approval of our product candidates. If our manufacturers or we are unable to purchase these key materials after regulatory approval has been obtained for our product candidates, the commercial launch of our product candidates would be delayed or there would be a shortage in supply, which would impair our ability to generate revenues from the sale of our product candidates.
Risks Related to Our Intellectual Property
If we are unable to obtain and maintain sufficient intellectual property protection for our product candidates, or if the scope of the intellectual property protection is not sufficiently broad, our ability to commercialize our product candidates successfully and to compete effectively may be adversely affected.
We rely upon a combination of patents, trade secrets and confidentiality agreements to protect the intellectual property related to our technology and product candidates. For our two most advanced molecularly targeted product candidates, PINTA 745 and STM 434, we own or license a number of issued patents and pending patent applications covering the product candidates’ compositions of matter and methods of use. For PINTA 745, the expected expiration dates range from 2026 to 2035 for US patents and patent applications, if issued, and from 2023 to 2035 for patents and patent applications, if issued, in jurisdictions outside the United States, exclusive of possible patent term extensions. For STM 434, the expected expiration dates range from 2027 through 2035 for US patents and patent applications, if issued, and from 2026 through 2035 for patents and patent applications, if issued, in jurisdictions outside the United States, exclusive of possible patent term extensions. The T-cell product candidates and platform technology we have licensed from MSK are protected primarily as confidential know-how and trade secrets. If we do not adequately protect our intellectual property, competitors may be able to use our technologies and erode or negate any competitive advantage we may have, which could harm our business and ability to achieve profitability. The patentability of inventions and the validity, enforceability and scope of patents in the biotechnology field is generally uncertain because it involves complex legal, scientific and factual considerations, and it has in recent years been the subject of significant litigation. Moreover, the standards applied by the US Patent and Trademark Office, or USPTO, and non-US patent offices in granting patents are not always applied uniformly or predictably. For example, there is no uniform worldwide policy regarding patentable subject matter or the scope of claims allowable in biotechnology patents.
Consequently, the patent applications that we own or in-license may fail to result in issued patents with claims that cover our product candidates in the United States or in other countries for many reasons. There is no assurance that all potentially relevant prior art relating to our patents and patent applications has been found. We may be unaware of prior art that could be used to invalidate an issued patent or prevent our pending patent applications from issuing as patents. There also may be prior art of which we are aware, but which we do not believe affects the validity or enforceability of a claim of one of our patents or patent applications, which may, nonetheless, ultimately be found to affect the validity or enforceability of such claim.
Even if patents have issued or do successfully issue from patent applications, and even if such patents cover our product candidates, third parties may challenge the validity, enforceability or scope thereof, which may result in such patents being narrowed, invalidated or held to be unenforceable. No assurance can be given that if challenged, our patents would be declared by a court to be valid or enforceable. Furthermore, even if they are unchallenged, our patents and patent applications may not adequately protect our intellectual property, provide exclusivity for our product candidates or prevent others from designing around our claims. The possibility exists that others will develop products on an independent basis which have the same effect as our product candidates and which do not infringe our
29
patents or other intellectual property rights, or that others will design around the claims of patents that we have had issued that cover our product candidates. If the breadth or strength of protection provided by the patents and patent applications we hold, license or pursue with respect to our product candidates is threatened, it could threaten our ability to commercialize our product candidates. In addition, the USPTO and various foreign governmental patent agencies require compliance with a number of procedural, documentary, fee payment and other similar provisions during the patent application process. While an inadvertent lapse can in many cases be cured by payment of a late fee or by other means in accordance with the applicable rules, there are situations in which noncompliance can result in abandonment or lapse of the patent or patent application, resulting in partial or complete loss of patent rights in the relevant jurisdiction. Any of these outcomes could have an adverse impact on our business.
If patent applications that we hold or in-license with respect to our technology or product candidates fail to issue, if their breadth or strength of protection is threatened, or if they fail to provide meaningful exclusivity for our product candidates, it could dissuade companies from collaborating with us. We have recently filed several patent applications covering our product candidates. We cannot offer any assurances about which, if any, patents will be issued with respect to these pending patent applications, the breadth of any such patents, whether any issued patents will be found invalid and unenforceable or will be threatened by third parties. Any successful challenge to these patents or any other patents owned by or exclusively licensed to us could deprive us of rights necessary for the successful commercialization of any product candidate that we or our collaborators may develop. Because patent applications in the United States and most other countries are confidential for a period of time after filing, and some remain so until issued, we cannot be certain that we were the first to file any patent application related to a product candidate. Furthermore, if third parties have filed such patent applications, an interference proceeding in the United States can be initiated by the USPTO or a third party to determine who was the first to invent any of the subject matter covered by the patent claims of our applications. Similarly, we could become involved in derivation proceedings before the USPTO to determine inventorship with respect to our patent applications. We may also become involved in similar opposition proceedings in the European Patent Office or counterpart offices in other jurisdictions regarding our intellectual property rights. In addition, patents have a limited lifespan. In the United States, the natural expiration of a patent generally occurs 20 years after it is filed. Although various extensions may be available if certain conditions are met, the life of a patent and the protection it affords is limited. If we encounter delays in our clinical trials or in obtaining regulatory approvals, the period of time during which we could exclusively market any of our product candidates under patent protection, if approved, could be reduced. Even if patents covering our product candidates are obtained, once the patent life has expired for a product, we may be vulnerable to competition from biosimilar products. Any loss of patent protection could have a material adverse impact on our business. We may be unable to prevent competitors from entering the market with a product that is similar or identical to our product candidates, which could harm our business and ability to achieve profitability.
Furthermore, the research resulting in certain of our licensed patent rights and technology was funded by the US government. As a result, the government may have certain rights, or march-in rights, to such patent rights and technology. When new technologies are developed with government funding, the government generally obtains certain rights in any resulting patents, including a non-exclusive license authorizing the government to use the invention for non-commercial purposes. These rights may permit the government to disclose our confidential information to third parties and to exercise march-in rights to use or allow third parties to use our licensed technology. The government can exercise its march-in rights if it determines that action is necessary because we fail to achieve practical application of the government-funded technology, because action is necessary to alleviate health or safety needs, to meet requirements of federal regulations or to give preference to US industry. In addition, our rights in such inventions may be subject to certain requirements to manufacture products embodying such inventions in the United States. Any exercise by the government of such rights could harm our competitive position, business, results of operations, financial condition and future prospects.
30
If we are sued for infringing the intellectual property rights of third parties, such litigation could be costly and time-consuming and could prevent or delay our development and commercialization efforts.
Our commercial success depends, in part, on us and our collaborators not infringing the patents and proprietary rights of third parties. There is a substantial amount of litigation, both within and outside the United States, involving patent and other intellectual property rights in the biotechnology and pharmaceutical industries, including patent infringement lawsuits, interference or derivation proceedings, oppositions, inter partes reexamination and review proceedings before the USPTO and corresponding non-US patent offices. Numerous US and non-US issued patents and pending patent applications owned by third parties exist in the fields in which we are developing and may develop our product candidates. As the biotechnology and pharmaceutical industries expand and more patents are issued, the risk increases that our product candidates may be subject to claims of infringement of third parties’ patent rights as it may not always be clear to industry participants, including us, which patents cover various types of products or methods of use. The coverage of patents is subject to interpretation by the courts, and the interpretation is not always uniform or predictable.
Third parties may assert infringement claims against us based on existing or future intellectual property rights, alleging that we are employing their proprietary technology without authorization. There may be third-party patents or patent applications with claims to materials, formulations, methods of manufacture or methods for treatment related to the use or manufacturing of our product candidates that we failed to identify. For example, applications filed before November 29, 2000, and certain applications filed after that date that will not be filed outside the United States, remain confidential until issued as patents. Except for the preceding exceptions, patent applications in the United States and elsewhere are generally published only after a waiting period of approximately 18 months after the earliest filing date. Therefore, patent applications covering our product candidates could have been filed by others without our knowledge. In addition, pending patent applications that have been published, including some of which we are aware, could be later amended in a manner that could cover our product candidates or their use or manufacture. We may analyze patents or patent applications of our competitors that we believe are relevant to our activities and believe that we are free to operate in relation to any of our product candidates, but our competitors may obtain issued claims, including in patents we consider to be unrelated, which may block our efforts or potentially result in any of our product candidates or our activities infringing such claims. If we are sued for patent infringement, we would need to demonstrate that our product candidates, products and methods either do not infringe the patent claims of the relevant patent or that the patent claims are invalid, and we may not be able to do this. Proving that a patent is invalid is difficult. For example, in the United States, proving invalidity requires a showing of clear and convincing evidence to overcome the presumption of validity enjoyed by issued patents. Even if we are successful in these proceedings, we may incur substantial costs and the time and attention of our management and scientific personnel could be diverted, which could have a material adverse effect on us. If any issued third-party patents were held by a court of competent jurisdiction to cover aspects of our materials, formulations, methods of manufacture or methods for treatment, we could be forced, including by court order, to cease developing, manufacturing or commercializing the relevant product candidate until such patent expired. Alternatively, we may be required to obtain a license from such third party in order to use the infringing technology and to continue developing, manufacturing or marketing the infringing product candidate. However, we may not be able to obtain any required license on commercially reasonably terms, or at all. Even if we were able to obtain a license, the rights may be nonexclusive, which could result in our competitors gaining access to the same intellectual property licensed to us. Ultimately, we could be prevented from commercializing a product candidate, or be forced to cease some aspect of our business operations, if, as a result of actual or threatened patent infringement claims, we are unable to enter into licenses on acceptable terms. This could harm our business significantly.
31
Parties making claims against us may obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our product candidates. Defending against claims of patent infringement or misappropriation of trade secrets could be costly and time consuming, regardless of the outcome. Thus, even if we were to ultimately prevail, or to settle at an early stage, such litigation could burden us with substantial unanticipated costs. In addition, litigation or threatened litigation could result in significant demands on the time and attention of our management team, distracting them from the pursuit of other company business. In the event of a successful claim of infringement against us, we may have to pay substantial damages, including treble damages and attorneys’ fees if we are found to have willfully infringed a patent, or to redesign our infringing product candidates which may be impossible or require substantial time and monetary expenditure. We may also elect to enter into license agreements in order to settle patent infringement claims prior to litigation, and any such license agreement may require us to pay royalties and other fees that could be significant.
We may face claims that we misappropriated the confidential information or trade secrets of a third party. If we are found to have misappropriated a third party’s trade secrets, we may be prevented from further using such trade secrets, which could limit our ability to develop our product candidates. We are not aware of any material threatened or pending claims related to these matters, but in the future litigation may be necessary to defend against such claims. If we fail in defending any such claims, in addition to paying monetary damages, we may lose valuable intellectual property rights or personnel. Even if we are successful in defending against such claims, litigation could result in substantial costs and be a distraction to management. During the course of any patent or other intellectual property litigation, there could be public announcements of the results of hearings, rulings on motions, and other interim proceedings in the litigation. If securities analysts or investors regard these announcements as negative, the perceived value of our product candidates, programs or intellectual property could be diminished. Accordingly, the market price of our common stock may decline.
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting, enforcing and defending patents on all of our product candidates in all countries throughout the world would be prohibitively expensive. Our or our licensors’ intellectual property rights in certain countries outside the United States may be less extensive than those in the United States. In addition, the laws of certain foreign countries do not protect intellectual property rights to the same extent as laws in the United States. Consequently, we and our licensors may not be able to prevent third parties from practicing our and our licensors’ inventions in countries outside the United States, or from selling or importing infringing products made using our and our licensors’ inventions in and into the United States or other jurisdictions. Competitors may use our and our licensors’ technologies in jurisdictions where we have not obtained patent protection to develop their own products and, further, may export otherwise infringing products to territories where we and our licensors have patent protection but where enforcement is not as strong as that in the United States. These infringing products may compete with our product candidates in jurisdictions where we or our licensors have no issued patents and our patent claims and other intellectual property rights may not be effective or sufficient to prevent them from so competing. Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents and other intellectual property protection, particularly those relating to biopharmaceuticals, which could make it difficult for us and our licensors to stop the infringement of our and our licensors’ patents or marketing of competing products in violation of our and our licensors’ proprietary rights generally. Proceedings to enforce our and our licensors’ patent rights in foreign jurisdictions could result in substantial costs and divert our attention from other aspects of our business, could put our and our licensors’ patents at risk of being invalidated or interpreted narrowly,
32
could put our and our licensors’ patent applications at risk of not issuing, and could provoke third parties to assert claims against us or our licensors. We or our licensors may not prevail in any lawsuits that we or our licensors initiate, and even if we or our licensors are successful the damages or other remedies awarded, if any, may not be commercially meaningful.
We have in-licensed a significant portion of our intellectual property from Amgen and MSK. If we breach any of our license agreements with Amgen or MSK, we could lose the ability to continue the development and potential commercialization of one or more of our product candidates.
We hold rights under a number of license agreements with Amgen and MSK that are important to our business. Our discovery and development platform is built, in part, around patent rights exclusively in-licensed from Amgen and MSK. The Amgen agreements generally grant us an exclusive (except as to the licenses to Amgen know-how, which are non-exclusive and limited as to their field of use), worldwide (except with regard to PINTA 745 in Japan, which was previously licensed to Takeda Pharmaceutical Company Limited) license to research, develop, improve, make, use, offer for sale, sell, import, export or otherwise exploit several classes of novel compounds, including PINTA 745 and STM 434. The MSK agreement generally grants us an exclusive license to research, develop, make, use, offer for sale, sell and import, EBV-CTL, CMV-CTL and WT1-CTL. Under our existing Amgen and MSK license agreements, we are subject to various obligations, including diligence obligations with respect to development and commercialization activities, payment obligations upon achievement of certain milestones and royalties on product sales, as well as other material obligations. If there is any conflict, dispute, disagreement or issue of nonperformance between us and Amgen or MSK regarding our rights or obligations under the license agreements, including any such conflict, dispute or disagreement arising from our failure to satisfy diligence or payment obligations under any such agreement, we may be liable to pay damages and Amgen or MSK may have a right to terminate the affected license. The loss of any or all of our license agreements with Amgen or our license agreement with MSK could materially adversely affect our ability to proceed to utilize the affected intellectual property in our drug discovery and development efforts, our ability to enter into future collaboration, licensing and/or marketing agreements for one or more affected product candidates and our ability to commercialize the affected product candidates. The risks described elsewhere pertaining to our patents and other intellectual property rights also apply to the intellectual property rights that we license, and any failure by us or our licensors to obtain, maintain and enforce these rights could have a material adverse effect on our business.
We may become involved in lawsuits to protect or enforce our intellectual property, which could be expensive, time-consuming and unsuccessful and have a material adverse effect on the success of our business and on our stock price.
Third parties may infringe our patents, the patents of our licensors, or misappropriate or otherwise violate our or our licensors’ intellectual property rights. Our and our licensors’ patent applications cannot be enforced against third parties practicing the technology claimed in such applications unless and until a patent issues from such applications, and then only to the extent the issued claims cover the technology. In the future, we or our licensors may elect to initiate legal proceedings to enforce or defend our or our licensors’ intellectual property rights, to protect our or our licensors’ trade secrets or to determine the validity or scope of intellectual property rights we own or control. Any claims that we assert against perceived infringers could also provoke these parties to assert counterclaims against us alleging that we infringe their intellectual property rights. In addition, third parties may initiate legal proceedings against us or our licensors to challenge the validity or scope of intellectual property rights we own or control. The proceedings can be expensive and time-consuming. Many of our or our licensors’ adversaries in these proceedings may have the ability to dedicate substantially greater resources to prosecuting these legal actions than we or our licensors can. Accordingly, despite our or
33
our licensors’ efforts, we or our licensors may not be able to prevent third parties from infringing upon or misappropriating intellectual property rights we own or control, particularly in countries where the laws may not protect our rights as fully as in the United States. Litigation could result in substantial costs and diversion of management resources, which could harm our business and financial results. In addition, in an infringement proceeding, a court may decide that a patent owned by or licensed to us is invalid or unenforceable, in whole or in part, or may refuse to stop the other party from using the technology at issue on the grounds that our or our licensors’ patents do not cover the technology in question. An adverse result in any litigation proceeding could put one or more of our or our licensors’ patents at risk of being invalidated, held unenforceable or interpreted narrowly.
Interference or derivation proceedings provoked by third parties, brought by us or our licensors or collaborators, or brought by the USPTO or any non-US patent authority may be necessary to determine the priority of inventions or other matters of inventorship with respect to our patents or patent applications. We may also become involved in other proceedings, such as reexamination or opposition proceedings, inter partes review or other preissuance or post-grant proceedings in the USPTO or its foreign counterparts relating to our intellectual property or the intellectual property rights of others. An unfavorable outcome in any such proceeding could require us or our licensors to cease using the related technology and commercializing our product candidates, or to attempt to license rights to it from the prevailing party. Our business could be harmed if the prevailing party does not offer us or our licensors a license on commercially reasonable terms if any license is offered at all. Even if we or our licensors obtain a license, it may be non-exclusive, thereby giving our competitors access to the same technologies licensed to us or our licensors. In addition, if the breadth or strength of protection provided by our or our licensors’ patents and patent applications is threatened, it could dissuade companies from collaborating with us to license, develop or commercialize current or future product candidates. Even if we successfully defend such litigation or proceeding, we may incur substantial costs and it may distract our management and other employees. We could be found liable for monetary damages, including treble damages and attorneys’ fees, if we are found to have willfully infringed a patent.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of shares of our common stock.
Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect our product candidates.
As is the case with other biotechnology and pharmaceutical companies, our success is heavily dependent on intellectual property, particularly patents. Obtaining and enforcing patents in the biopharmaceutical industry involves both technological and legal complexity, and obtaining and enforcing biopharmaceutical patents is costly, time-consuming, and inherently uncertain. The Supreme Court has ruled on several patent cases in recent years, either narrowing the scope of patent protection available in certain circumstances or weakening the rights of patent owners in certain situations. In addition to increasing uncertainty with regard to our and our licensors’ ability to obtain patents in the future, this combination of events has created uncertainty with respect to the value of patents once obtained. Depending on future decisions by the US Congress, or Congress, the federal courts and the USPTO, the laws and regulations governing patents could change in unpredictable ways that may weaken our and our licensors’ ability to obtain new patents or to enforce existing patents and patents we and our licensors or collaborators may obtain in the future.
34
Recent patent reform legislation could increase the uncertainties and costs surrounding the prosecution of our and our licensors’ patent applications and the enforcement or defense of our or our licensors’ issued patents. On September 16, 2011, the Leahy-Smith America Invents Act, or the Leahy-Smith Act, was signed into law. The Leahy-Smith Act includes a number of significant changes to US patent law. These include provisions that affect the way patent applications are prosecuted and may also affect patent litigation. The USPTO recently developed new regulations and procedures to govern administration of the Leahy-Smith Act, and many of the substantive changes to patent law associated with the Leahy-Smith Act, and in particular, the first to file provisions, only became effective on March 16, 2013. Accordingly, it is not clear what, if any, impact the Leahy-Smith Act will have on the operation of our business. However, the Leahy-Smith Act and its implementation could increase the uncertainties and costs surrounding the prosecution of our or our licensors’ patent applications and the enforcement or defense of our or our licensors’ issued patents, all of which could have a material adverse effect on our business and financial condition.
If we are unable to protect the confidentiality of our trade secrets and other proprietary information, the value of our technology could be materially adversely affected and our business could be harmed.
In addition to seeking the protection afforded by patents, we rely on trade secret protection and confidentiality agreements to protect proprietary know-how that is not patentable or that we elect not to patent, processes for which patents are difficult to enforce, and other elements of our technology, discovery and development processes that involve proprietary know-how, information or technology that is not covered by patents. The T-cell product candidates and platform technology we have licensed from MSK are protected primarily as confidential know-how and trade secrets. Any disclosure to or misappropriation by third parties of our confidential proprietary information could enable competitors to quickly duplicate or surpass our technological achievements, including by enabling them to develop and commercialize products substantially similar to or competitive with our EBV-CTL, CMV-CTL or WT1 product candidates, thus eroding our competitive position in the market. However, trade secrets can be difficult to protect. We seek to protect our proprietary technology and processes, in part, by entering into confidentiality agreements and invention assignment agreements with our employees, consultants, and outside scientific advisors, contractors and collaborators. These agreements are designed to protect our proprietary information. Although we use reasonable efforts to protect our trade secrets, our employees, consultants, contractors, or outside scientific advisors might intentionally or inadvertently disclose our trade secrets or confidential, proprietary information to competitors. In addition, competitors may otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. If any of our confidential proprietary information were to be lawfully obtained or independently developed by a competitor, we would have no right to prevent such competitor from using that technology or information to compete with us, which could harm our competitive position.
Enforcing a claim that a third party illegally obtained and is using any of our trade secrets is expensive and time consuming, and the outcome is unpredictable. In addition, the laws of certain foreign countries do not protect proprietary rights such as trade secrets to the same extent or in the same manner as the laws of the United States. Misappropriation or unauthorized disclosure of our trade secrets to third parties could impair our competitive advantage in the market and could materially adversely affect our business, results of operations and financial condition.
35
Risks Related to Commercialization of Our Product Candidates
Our commercial success depends upon attaining significant market acceptance of our product candidates, if approved, among physicians, patients, healthcare payors and major operators of dialysis and cancer clinics.
Even if we obtain regulatory approval for any of our product candidates that we may develop or acquire in the future, the product may not gain market acceptance among physicians, healthcare payors, patients or the medical community, including major operators of dialysis and cancer clinics. Market acceptance of any of our product candidates for which we receive approval depends on a number of factors, including:
| • | the efficacy and safety of such product candidates as demonstrated in clinical trials; |
| • | the clinical indications for which the product candidate is approved; |
| • | acceptance by physicians, major operators of cancer and dialysis clinics and patients of the drug as a safe and effective treatment; |
| • | the adoption of novel cellular therapies by physicians, hospitals and third-party payors; |
| • | the potential and perceived advantages of product candidates over alternative treatments; |
| • | the safety of product candidates seen in a broader patient group, including its use outside the approved indications; |
| • | any restrictions on use together with other medications; |
| • | the prevalence and severity of any side effects; |
| • | product labeling or product insert requirements of the FDA or other regulatory authorities; |
| • | the timing of market introduction of our products as well as competitive products; |
| • | the development of manufacturing and distribution processes for our novel T-cell product candidates; |
| • | the cost of treatment in relation to alternative treatments; |
| • | the availability of coverage and adequate reimbursement and pricing by third-party payors and government authorities; |
| • | relative convenience and ease of administration; and |
| • | the effectiveness of our sales and marketing efforts and those of our collaborators. |
If any of our product candidates are approved but fail to achieve market acceptance among physicians, patients, healthcare payors or major operators of dialysis and cancer clinics, we will not be able to generate significant revenues, which would compromise our ability to become profitable. In particular, the dialysis industry is dominated by two companies, DaVita Healthcare Partners and Fresenius. In the event PINTA 745 fails to be accepted by either of these companies, our ability to generate revenues from PINTA 745 and become profitable would be adversely affected.
Even if we are able to commercialize our product candidates, the products may not receive coverage and adequate reimbursement from third-party payors in the United States and in other countries in which we seek to commercialize our products, which could harm our business.
Our ability to commercialize any product successfully will depend, in part, on the extent to which coverage and adequate reimbursement for these products and related treatments will be available from government health administration authorities, private health insurers and other organizations.
36
Government authorities and third-party payors, such as private health insurers and health maintenance organizations, determine which medications they will cover and establish reimbursement levels. A primary trend in the healthcare industry is cost containment. Government authorities and third-party payors have attempted to control costs by limiting coverage and the amount of reimbursement for particular medications. Increasingly, third-party payors are requiring that drug companies provide them with predetermined discounts from list prices and are challenging the prices charged for medical products. Third-party payors may also seek additional clinical evidence, beyond the data required to obtain regulatory approval, demonstrating clinical benefits and value in specific patient populations before covering our products for those patients. We cannot be sure that coverage and adequate reimbursement will be available for any product that we commercialize and, if reimbursement is available, what the level of reimbursement will be. Coverage and reimbursement may impact the demand for, or the price of, any product candidate for which we obtain regulatory approval. If reimbursement is not available or is available only at limited levels, we may not be able to successfully commercialize any product candidate for which we obtain regulatory approval.
There may be significant delays in obtaining coverage and reimbursement for newly approved drugs, and coverage may be more limited than the purposes for which the drug is approved by the FDA or comparable foreign regulatory authorities. Moreover, eligibility for coverage and reimbursement does not imply that any drug will be paid for in all cases or at a rate that covers our costs, including research, development, manufacture, sale and distribution. Interim reimbursement levels for new drugs, if applicable, may also not be sufficient to cover our costs and may only be temporary. Reimbursement rates may vary according to the use of the drug and the clinical setting in which it is used, may be based on reimbursement levels already set for lower cost drugs and may be incorporated into existing payments for other services. Net prices for drugs may be reduced by mandatory discounts or rebates required by government healthcare programs or private payors and by any future relaxation of laws that presently restrict imports of drugs from countries where they may be sold at lower prices than in the United States. Third-party payors in the United States often rely upon Medicare coverage policy and payment limitations in setting their own reimbursement policies. Our inability to promptly obtain coverage and profitable reimbursement rates from both government-funded and private payors for any approved products that we develop could have a material adverse effect on our operating results, our ability to raise capital needed to commercialize products and our overall financial condition.
Recently enacted and future legislation, including potentially unfavorable pricing regulations or other healthcare reform initiatives, may increase the difficulty and cost for us to obtain regulatory approval of and commercialize our product candidates and affect the prices we may obtain.
The regulations that govern, among other things, regulatory approvals, coverage, pricing and reimbursement for new drug products vary widely from country to country. In the United States and some foreign jurisdictions, there have been a number of legislative and regulatory changes and proposed changes regarding the healthcare system that could prevent or delay regulatory approval of our product candidates, restrict or regulate post-approval activities and affect our ability to successfully sell any product candidates for which we obtain regulatory approval.
In the United States, the Medicare Prescription Drug, Improvement, and Modernization Act of 2003, or Medicare Modernization Act, changed the way Medicare covers and pays for pharmaceutical products. The legislation expanded Medicare coverage for drug purchases by the elderly and introduced a new reimbursement methodology based on average sales prices for physician- administered drugs. In particular, all Medicare payments for dialysis treatments to ESRD patients are now made under a single bundled payment rate that provides a fixed payment rate to encompass all goods and services provided during the dialysis treatment, including pharmaceuticals that were
37
historically separately reimbursed to the dialysis providers, irrespective of the level of pharmaceuticals administered or additional services performed. Most lab services that used to be paid directly to laboratories are also included in the bundled payment. Unless we are able to secure an exemption, PINTA 745 may be subject to the bundled payment system. In recent years, Congress has considered further reductions in Medicare reimbursement for drugs administered by physicians. The Center for Medicare and Medicaid Services, or CMS, the agency that runs the Medicare program, also has the authority to revise reimbursement rates, including under the bundled payment system, and to implement coverage restrictions for some drugs. Cost reduction initiatives and changes in coverage implemented through legislation or regulation could decrease utilization of and reimbursement for any approved products, which in turn would affect the price we can receive for those products. While the Medicare Modernization Act and Medicare regulations apply only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own reimbursement rates. Therefore, any reduction in reimbursement that results from federal legislation or regulation may result in a similar reduction in payments from private payors.
In March 2010, President Obama signed into law the Patient Protection and Affordable Care Act and the Health Care and Education Affordability Reconciliation Act of 2010, or the Affordable Care Act, a sweeping law intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on pharmaceutical and medical device manufacturers and impose additional health policy reforms. The Affordable Care Act expanded manufacturers’ rebate liability to include covered drugs dispensed to individuals who are enrolled in Medicaid managed care organizations, increased the minimum rebate due for innovator drugs from 15.1% of average manufacturer price, or AMP, to 23.1% of AMP, and capped the total rebate amount for innovator drugs at 100% of AMP. The Affordable Care Act and subsequent legislation also changed the definition of AMP. Furthermore, the Affordable Care Act imposes a significant annual, nondeductible fee on companies that manufacture or import certain branded prescription drug products. Substantial new provisions affecting compliance have also been enacted, which may affect our business practices with healthcare practitioners, and a significant number of provisions are not yet, or have only recently become, effective. Although it is too early to determine the effect of the Affordable Care Act, it appears likely to continue the pressure on pharmaceutical pricing, especially under the Medicare program, and may also increase our regulatory burdens and operating costs.
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. More recently, in August 2011, the President signed into law the Budget Control Act of 2011, which, among other things, creates the Joint Select Committee on Deficit Reduction to recommend to Congress proposals in spending reductions. The Joint Select Committee did not achieve a targeted deficit reduction of at least $1.2 trillion for the years 2013 through 2021, triggering the legislation’s automatic reduction to several government programs. This includes aggregate reductions to Medicare payments to providers of up to 2% per fiscal year, starting in 2013. In January 2013, President Obama signed into law the American Taxpayer Relief Act of 2012, which, among other things, reduced Medicare payments to several providers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. In March 2013, the President signed an executive order implementing sequestration, and in April 2013, the 2% Medicare reductions went into effect. These new laws may result in additional reductions in Medicare and other healthcare funding, which could have a material adverse effect on our customers and accordingly, our financial operations. Legislative and regulatory proposals have been made to expand post-approval requirements and restrict sales and promotional activities for pharmaceutical products. We cannot be sure whether additional legislative changes will be enacted, or whether the FDA regulations, guidance or interpretations will be changed, or what the impact of such changes on the regulatory approvals of our product candidates, if any, may be.
38
In the United States, the European Union and other potentially significant markets for our product candidates, government authorities and third-party payors are increasingly attempting to limit or regulate the price of medical products and services, particularly for new and innovative products and therapies, which has resulted in lower average selling prices. Furthermore, the increased emphasis on managed healthcare in the United States and on country and regional pricing and reimbursement controls in the European Union will put additional pressure on product pricing, reimbursement and usage, which may adversely affect our future product sales and results of operations. These pressures can arise from rules and practices of managed care groups, judicial decisions and governmental laws and regulations related to Medicare, Medicaid and healthcare reform, pharmaceutical reimbursement policies and pricing in general.
Price controls may be imposed in foreign markets, which may adversely affect our future profitability.
In some countries, particularly member states of the European Union, the pricing of prescription drugs is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after receipt of regulatory approval for a product. In addition, there can be considerable pressure by governments and other stakeholders on prices and reimbursement levels, including as part of cost containment measures. Political, economic and regulatory developments may further complicate pricing negotiations, and pricing negotiations may continue after reimbursement has been obtained. Reference pricing used by various European Union member states and parallel distribution, or arbitrage between low-priced and high-priced member states, can further reduce prices. In some countries, we or our collaborators may be required to conduct a clinical trial or other studies that compare the cost-effectiveness of our product candidates to other available therapies in order to obtain or maintain reimbursement or pricing approval. Publication of discounts by third-party payors or authorities may lead to further pressure on the prices or reimbursement levels within the country of publication and other countries. If reimbursement of our products is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, our business could be adversely affected.
We face substantial competition, which may result in others discovering, developing or commercializing products before or more successfully than we do.
We face competition from numerous pharmaceutical and biotechnology enterprises, as well as from academic institutions, government agencies and private and public research institutions for our current product candidates. Our commercial opportunities will be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer side effects or are less expensive than any products that we may develop. Competition could result in reduced sales and pricing pressure on our product candidates, if approved, which in turn would reduce our ability to generate meaningful revenues and have a negative impact on our results of operations. In addition, significant delays in the development of our product candidates could allow our competitors to bring products to market before us and impair any ability to commercialize our product candidates.
Products are currently marketed or used off-label for the muscle wasting-related indications for which the products in our pipeline are being developed, and a number of companies are or may be developing new treatments for muscle wasting indications. These products, as well as promotional efforts by competitors and clinical trial results of competitive products, could significantly diminish any ability to market and sell PINTA 745 and other product candidates focused on muscle wasting-related indications. Today’s treatment for protein-energy wasting and cancer cachexia often involves the administration of readily available nutritional supplements and appetite stimulants including, in some jurisdictions, medical marijuana. In addition, there are two commercially available steroids, nandrolone and oxandrolone, that are sometimes prescribed off-label for the treatment of weight loss in cancer
39
patients. A number of companies are developing drug candidates for muscle wasting applications, including, but not limited to: Eli Lilly & Co., which is conducting Phase 1 clinical studies and Phase 2 clinical trials for LY2495655, and Pfizer Inc., which is conducting Phase 1 clinical studies for PF-06252616, both of which are myostatin antibodies, to evaluate their ability to increase and improve muscle mass in various patient populations; Novartis Corporation, which is conducting Phase 1 clinical studies and Phase 2 clinical trials for BYM338, an ActR2B antibody, to evaluate its ability to build muscle in patients with various muscle-wasting conditions; Ligand Pharmaceuticals, which is developing LGD-4033, a selective androgen receptor modulator, for muscle wasting; Regeneron Pharmaceuticals, Inc., which is developing REGN1033, a myostatin antibody, in collaboration with Sanofi-Aventis for sarcopenia; Acceleron Pharma, Inc., which is developing ACE-083, a modified cysteine knot ligand trap of the TGF-ß superfamily, for diseases in which improved muscle strength may provide a clinical benefit, such as inclusion body myositis and certain forms of muscular dystrophy; and GTx, Inc., which is developing ostarine, a selective androgen receptor modulator for cachexia.
There are numerous approved products and therapies for ovarian cancer, and a number of companies are or may be developing new treatments for ovarian cancer and other solid tumors. These therapies, as well as promotional efforts by competitors and clinical trial results of competitive products, could significantly diminish any ability to market and sell STM 434. Approved drug therapies for ovarian cancer include: chemotherapy with platinum compounds such as cisplatin or carboplatin and taxane compounds such as paclitaxel or docetaxel; bevacizumab in combination with a chemotherapy compound such as liposomal doxorubicin, paclitaxel or topotecan; olaparib in patients with deleterious or suspected deleterious germline breast cancer susceptibility gene, known as BRCA, mutated advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy; and hormone therapies including goserelin, leuprolide, tamoxifen, letrozole, anastrozole and exemestane. A number of companies are developing drug candidates for ovarian cancer and other solid tumors, including, but not limited to Genentech/Roche, which is developing bevacizumab (Avastin) and other potential drug therapies.
There currently are no FDA or EMA approved products for the treatment of EBV-LPD. However, some approved products and therapies are used off-label in the treatment of EBV-LPD, such as rituximab and combination chemotherapy regimens. In addition, a number of companies and academic institutions are developing drug candidates for EBV-LPD and other EBV associated diseases including: Cell Medica Ltd., or Cell Medica, which is conducting Phase 2 clinical studies for Cytorex EBV, an autologous EBV specific T-cell therapy in NK/T-cell lymphoma; Adcyte LLC, or Adcyte, which has licensed multi-virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor and ViraCyte, which has licensed virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor.
Drug therapies approved or commonly used for CMV infection include antiviral compounds such as ganciclovir, valganciclovir, cidofovir and foscarnet. In addition, a number of companies and academic institutions are developing drug candidates for CMV infection and other CMV-associated diseases, including: Shire Plc, or Shire, which is conducting Phase 2 clinical trials of maribavir, a UL97 protein kinase inhibitor; Merck & Co. Inc., or Merck, which is conducting Phase 3 clinical trials of letermovir, a CMV terminase inhibitor; Chimerix, Inc., or Chimerix, which is conducting Phase 3 clinical trials for brincidofovir, a lipid conjugated nucleotide analogue of cidofovir; Cell Medica, which is conducting Phase 3 clinical trials for Cytovir CMV, a CMV-specific cell therapy product derived from primary HCT transplant donors; Adcyte, which has licensed multi-virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor and ViraCyte, which has licensed virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor.
Many of the approved or commonly used drugs and therapies for muscle wasting, ovarian cancer, EBV-LPD and CMV are well-established and are widely accepted by physicians, patients and third-
40
party payors. Some of these drugs are branded and subject to patent protection, and other drugs and nutritional supplements are available on a generic basis. Insurers and other third-party payors may encourage the use of generic products or specific branded products. We expect that, if any of these product candidates is approved, it will be priced at a significant premium over competitive generic products. This pricing premium may make it difficult for us to differentiate these products from currently approved or commonly used therapies and impede adoption of our product, which may adversely impact our business. In addition, many companies are developing new therapeutics, and we cannot predict what the standard of care will become as our products continue in clinical development.
Many of our competitors or potential competitors have significantly greater established presence in the market, financial resources and expertise in research and development, manufacturing, preclinical testing, conducting clinical trials, obtaining regulatory approvals and marketing approved products than we do, and as a result may have a competitive advantage over us. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in recruiting and retaining qualified scientific and management personnel, establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies and technology licenses complementary to our programs or advantageous to our business.
As a result of these factors, these competitors may obtain regulatory approval of their products before we are able to obtain patent protection or other intellectual property rights, which will limit our ability to develop or commercialize our product candidates. Our competitors may also develop drugs that are safer, more effective, more widely used and cheaper than ours, and may also be more successful than us in manufacturing and marketing their products. These appreciable advantages could render our product candidates obsolete or noncompetitive before we can recover the expenses of development and commercialization.
Mergers and acquisitions in the pharmaceutical and biotechnology industries may result in even more resources being concentrated among a smaller number of our competitors. Smaller and other early stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large and established companies. These third parties compete with us in recruiting and retaining qualified scientific, management and commercial personnel, establishing clinical trial sites and patient registration for clinical trials, as well as in acquiring technologies complementary to, or necessary for, our programs.
If we are unable to establish sales and marketing capabilities or enter into agreements with third parties to market and sell our product candidates, we may be unable to generate any revenue.
We do not currently have an organization for the sale, marketing and distribution of pharmaceutical products and the cost of establishing and maintaining such an organization may exceed the cost-effectiveness of doing so. In order to market any products that may be approved by the FDA and comparable foreign regulatory authorities, we must build our sales, marketing, managerial and other non-technical capabilities or make arrangements with third parties to perform these services. There are significant risks involved in building and managing a sales organization, including our ability to hire, retain and incentivize qualified individuals, generate sufficient sales leads, provide adequate training to sales and marketing personnel and effectively manage a geographically dispersed sales and marketing team. Any failure or delay in the development of our internal sales, marketing and distribution capabilities would adversely impact the commercialization of these products. If we are unable to establish adequate sales, marketing and distribution capabilities, whether independently or with third parties, we may not be able to generate product revenues and may not become profitable. We will be competing with many companies that currently have extensive and well-funded sales and
41
marketing operations. Without an internal commercial organization or the support of a third party to perform sales and marketing functions, we may be unable to compete successfully against these more established companies. If we are not successful in commercializing our current or future product candidates either on our own or through collaborations with one or more third parties, our future product revenue will suffer and we would incur significant additional losses.
We will need to grow the size of our organization, and we may experience difficulties in managing this growth.
As of May 31, 2015, we had 29 employees. We need to grow the size of our organization in order to support our continued development and potential commercialization of our product candidates. In particular, we will need to add substantial numbers of additional personnel and other resources to support our development and potential commercialization of EBV-CTL, CMV-CTL and WT1-CTL as a result of our recent exercise of our option to license these programs from MSK. As our development and commercialization plans and strategies continue to develop, or as a result of any future acquisitions, our need for additional managerial, operational, manufacturing, sales, marketing, financial and other resources will increase. Our management, personnel and systems currently in place may not be adequate to support this future growth. Future growth would impose significant added responsibilities on members of management, including:
| • | managing our clinical studies and trials effectively; |
| • | identifying, recruiting, maintaining, motivating and integrating additional employees; |
| • | managing our internal development efforts effectively while complying with our contractual obligations to licensors, licensees, contractors and other third parties; |
| • | improving our managerial, development, operational, information technology, and finance systems; and |
| • | expanding our facilities. |
As our operations expand, we will also need to manage additional relationships with various strategic partners, suppliers and other third parties. Our future financial performance and our ability to commercialize our product candidates and to compete effectively will depend, in part, on our ability to manage any future growth effectively. To that end, we must be able to manage our development efforts and clinical studies and trials effectively and hire, train and integrate additional management, research and development, manufacturing, administrative and sales and marketing personnel. Our failure to accomplish any of these tasks could prevent us from successfully growing our company.
Our future success depends on our ability to retain our executive officers and to attract, retain and motivate qualified personnel.
We are highly dependent upon our personnel, including Isaac E. Ciechanover, M.D., our President, Chief Executive Officer and founder, and Christopher Haqq, Ph.D., M.D., our Chief Medical Officer. Our employment agreements with Drs. Ciechanover and Haqq are at-will and do not prevent them from terminating their employment with us at any time. The loss of the services of either of them could impede the achievement of our research, development and commercialization objectives.
Our future growth and success depend on our ability to recruit, retain, manage and motivate our employees. The loss of any member of our senior management team or the inability to hire or retain experienced management personnel could compromise our ability to execute our business plan and harm our operating results. Because of the specialized scientific and managerial nature of our business, we rely heavily on our ability to attract and retain qualified scientific, technical and managerial personnel. The competition for qualified personnel in the pharmaceutical field is intense and as a result, we may be unable to continue to attract and retain qualified personnel necessary for the development of our business.
42
Our relationships with customers and third-party payors will be subject to applicable anti-kickback, fraud and abuse and other healthcare laws and regulations, which could expose us to criminal sanctions, civil penalties, contractual damages, reputational harm and diminished profits and future earnings.
Healthcare providers, physicians and third-party payors will play a primary role in the recommendation and prescription of any product candidates for which we obtain regulatory approval. Our future arrangements with third-party payors and customers may expose us to broadly applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships through which we would market, sell and distribute our products. As a pharmaceutical company, even though we do not and will not control referrals of healthcare services or bill directly to Medicare, Medicaid or other third-party payors, federal and state healthcare laws and regulations pertaining to fraud and abuse and patients’ rights are and will be applicable to our business. Restrictions under applicable federal and state healthcare laws and regulations that may affect our ability to operate include the following:
| • | the federal healthcare Anti-Kickback Statute will constrain our marketing practices, educational programs, pricing policies, and relationships with healthcare providers or other entities, by prohibiting, among other things, persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward, or in return for, either the referral of an individual for, or the purchase, order or recommendation of, any good or service, for which payment may be made under a federal healthcare program such as Medicare and Medicaid; |
| • | federal civil and criminal false claims laws and civil monetary penalty laws impose criminal and civil penalties, including through civil whistleblower or qui tam actions, against individuals or entities for knowingly presenting, or causing to be presented, to the federal government, including the Medicare and Medicaid programs, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| • | the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, imposes criminal and civil liability for executing a scheme to defraud any healthcare benefit program and also created federal criminal laws that prohibit knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false statements in connection with the delivery of or payment for healthcare benefits, items or services; |
| • | HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH, also imposes obligations, including mandatory contractual terms, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
| • | the federal physician sunshine requirements under the Affordable Care Act requires manufacturers of drugs, devices, biologics and medical supplies to report annually to HHS information related to payments and other transfers of value to physicians, other healthcare providers, and teaching hospitals, and ownership and investment interests held by physicians and other healthcare providers and their immediate family members and applicable group purchasing organizations; and |
| • | analogous state and foreign laws and regulations, such as state anti-kickback and false claims laws, may apply to sales or marketing arrangements and claims involving healthcare items or services reimbursed by non-governmental third-party payors, including private insurers; some state laws require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government and may require drug manufacturers to report information related to payments and other transfers of value to physicians and other healthcare providers or |
43
| marketing expenditures; and state and foreign laws govern the privacy and security of health information in specified circumstances, many of which differ from each other in significant ways and often are not preempted by HIPAA, thus complicating compliance efforts. |
Efforts to ensure that our business arrangements with third parties will comply with applicable healthcare laws and regulations will involve substantial costs. It is possible that governmental authorities will conclude that our business practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of these laws or any other governmental regulations that may apply to us, we may be subject to significant civil, criminal and administrative penalties, damages, fines, imprisonment, exclusion from government funded healthcare programs, such as Medicare and Medicaid, and the curtailment or restructuring of our operations. If any physicians or other healthcare providers or entities with whom we expect to do business are found to not be in compliance with applicable laws, they may be subject to criminal, civil or administrative sanctions, including exclusions from government funded healthcare programs.
Our employees may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements, which could cause significant liability for us and harm our reputation.
We are exposed to the risk of employee fraud or other misconduct, including intentional failures to comply with FDA regulations or similar regulations of comparable foreign regulatory authorities, provide accurate information to the FDA or comparable foreign regulatory authorities, comply with manufacturing standards we have established, comply with federal and state healthcare fraud and abuse laws and regulations and similar laws and regulations established and enforced by comparable foreign regulatory authorities, report financial information or data accurately or disclose unauthorized activities to us. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. It is not always possible to identify and deter employee misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business and results of operations, including the imposition of significant fines or other sanctions.
Product liability lawsuits against us could cause us to incur substantial liabilities and to limit commercialization of any products that we may develop.
We face an inherent risk of product liability exposure related to the testing of our product candidates in human clinical trials and will face an even greater risk if we commercially sell any products that we may develop. Product liability claims may be brought against us by subjects enrolled in our clinical trials, patients, healthcare providers or others using, administering or selling our products. If we cannot successfully defend ourselves against claims that our product candidates or products caused injuries, we could incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
| • | decreased demand for any product candidates or products that we may develop; |
| • | termination of clinical trial sites or entire trial programs; |
| • | injury to our reputation and significant negative media attention; |
| • | withdrawal of clinical trial participants; |
44
| • | significant costs to defend the related litigation; |
| • | substantial monetary awards to trial subjects or patients; |
| • | loss of revenue; |
| • | diversion of management and scientific resources from our business operations; and |
| • | the inability to commercialize any products that we may develop. |
We currently hold $5.0 million in product liability insurance coverage in the aggregate, which we believe is customary for similarly situated companies and adequate to provide us with insurance coverage for foreseeable risks, but which may not be adequate to cover all liabilities that we may incur. Insurance coverage is increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost or in an amount adequate to satisfy any liability that may arise. We intend to expand our insurance coverage for products to include the sale of commercial products if we obtain regulatory approval for our product candidates in development, but we may be unable to obtain commercially reasonable product liability insurance for any products that receive regulatory approval. Large judgments have been awarded in class action lawsuits based on drugs that had unanticipated side effects. A successful product liability claim or series of claims brought against us, particularly if judgments exceed our insurance coverage, could decrease our cash and adversely affect our business.
If we and our third-party manufacturers fail to comply with environmental, health and safety laws and regulations, we could become subject to fines or penalties or incur costs that could have a material adverse effect on the success of our business.
We and our third-party manufacturers are subject to numerous environmental, health and safety laws and regulations, including those governing laboratory procedures and the handling, use, storage, treatment and disposal of hazardous materials and wastes. Our operations involve the use of hazardous and flammable materials, including chemicals and biological materials. Our operations also produce hazardous waste products. We generally contract with third parties for the disposal of these materials and wastes. We cannot eliminate the risk of contamination or injury from these materials. In the event of contamination or injury resulting from our or our third-party manufacturers’ use of hazardous materials, we could be held liable for any resulting damages, and any liability could exceed our resources. We also could incur significant costs associated with civil or criminal fines and penalties.
Although we maintain workers’ compensation insurance to cover us for costs and expenses we may incur due to injuries to our employees resulting from the use of hazardous materials with a policy limit that we believe is customary for similarly situated companies and adequate to provide us with insurance coverage for foreseeable risks, this insurance may not provide adequate coverage against potential liabilities. We do not maintain insurance for environmental liability or toxic tort claims that may be asserted against us in connection with our storage or disposal of biological or hazardous materials.
In addition, we may incur substantial costs in order to comply with current or future environmental, health and safety laws and regulations. These current or future laws and regulations may impair our research, development or production efforts. Failure to comply with these laws and regulations also may result in substantial fines, penalties or other sanctions.
Our business and operations would suffer in the event of computer system failures or security breaches.
Our internal computer systems, and those of MSK, our CROs and other business vendors on which we rely, are vulnerable to damage from computer viruses, unauthorized access, natural disasters, fire, terrorism, war and telecommunication and electrical failures. We exercise little or no
45
control over these third parties, which increases our vulnerability to problems with their systems. If such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our drug development programs. For example, the loss of clinical trial data from completed, ongoing or planned clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach results in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability, the further development of our product candidates could be delayed and our business could be otherwise adversely affected.
Business disruptions could seriously harm our future revenues and financial condition and increase our costs and expenses.
Our operations could be subject to earthquakes, power shortages, telecommunications failures, water shortages, floods, hurricanes, typhoons, fires, extreme weather conditions, medical epidemics and other natural or manmade disasters or business interruptions, for which we are predominantly self-insured. The occurrence of any of these business disruptions could seriously harm our operations and financial condition and increase our costs and expenses. We rely on third-party manufacturers to produce our product candidates. Our ability to obtain clinical supplies of product candidates could be disrupted, if the operations of these suppliers are affected by a man-made or natural disaster or other business interruption. The ultimate impact on us, our significant suppliers and our general infrastructure is unknown, but our operations and financial condition could suffer in the event of a major earthquake, fire or other natural disaster.
Risks Related to This Offering and Ownership of Our Common Stock
Our stock price has been and will likely continue to be volatile and may decline regardless of our operating performance.
Our stock price has fluctuated in the past and can be expected to be volatile in the future. From October 16, 2014, the first date of trading of our common stock, through June 26, 2015, the reported sale price of our common stock has fluctuated between $9.66 and $64.35 per share. The stock market in general and the market for biotechnology companies in particular have experienced extreme volatility that has often been unrelated to the operating performance of particular companies. As a result of this volatility, investors may experience losses on their investment in our common stock. The market price of our common stock may be influenced by many factors, including the following:
| • | the success of competitive products or technologies; |
| • | regulatory actions with respect to our product candidates or products or our competitors’ product candidates or products; |
| • | actual or anticipated changes in our growth rate relative to our competitors; |
| • | announcements by us or our competitors of significant acquisitions, strategic partnerships, joint ventures, collaborations or capital commitments; |
| • | results of clinical trials of our product candidates or those of our competitors; |
| • | regulatory or legal developments in the United States and other countries; |
| • | developments or disputes concerning patent applications, issued patents or other proprietary rights; |
| • | the recruitment or departure of key personnel; |
| • | the level of expenses related to any of our product candidates or clinical development programs; |
46
| • | the results of our efforts to in-license or acquire additional product candidates or products; |
| • | actual or anticipated changes in estimates as to financial results, development timelines or recommendations by securities analysts; |
| • | variations in our financial results or those of companies that are perceived to be similar to us; |
| • | fluctuations in the valuation of companies perceived by investors to be comparable to us; |
| • | inconsistent trading volume levels of our shares; |
| • | announcement or expectation of additional financing efforts; |
| • | sales of our common stock by us, our insiders or our other stockholders; |
| • | changes in the structure of healthcare payment systems; |
| • | market conditions in the pharmaceutical and biotechnology sectors; |
| • | general economic, industry and market conditions; and |
| • | the other risks described in this “Risk Factors” section. |
We may be subject to securities litigation, which is expensive and could divert management attention.
The market price of our common stock has been volatile, and in the past companies that have experienced volatility in the market price of their stock have been subject to securities class action litigation. We may be the target of this type of litigation in the future. Securities litigation against us could result in substantial costs and divert our management’s attention from other business concerns, which could seriously harm our business.
Our principal stockholders and management own a significant percentage of our stock and will be able to exert significant control over matters subject to stockholder approval.
As of May 31, 2015, our executive officers, directors, holders of 5% or more of our capital stock and their respective affiliates together owned more than 70% of our outstanding voting stock, assuming no exercise of outstanding options. These stockholders may be able to determine the outcome of all matters requiring stockholder approval. For example, these stockholders may be able to control elections of directors, amendments of our organizational documents, or approval of any merger, sale of assets, or other major corporate transaction. This may prevent or discourage unsolicited acquisition proposals or offers for our common stock that you may feel are in your best interest as one of our stockholders. The interests of this group of stockholders may not always coincide with your interests or the interests of other stockholders and they may act in a manner that advances their best interests and not necessarily those of other stockholders, including seeking a premium value for their common stock, and might affect the prevailing market price for our common stock.
Sales of a substantial number of shares of our common stock in the public market could cause our stock price to fall.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock. After this offering, we will have shares of common stock outstanding based on (i) 24,525,822 shares outstanding as of May 31, 2015 and (ii) the shares that we are selling in this offering. The shares that we are selling in this offering may be resold in the public market immediately without restriction, unless purchased by our directors or officers or our stockholders who are subject to a lock-up agreement. Of
47
the remaining shares, shares of our common stock will be restricted as a result of lock-up agreements but will be able to be sold after the offering as described in the “Shares Eligible for Future Sale” section of this prospectus. Moreover, certain holders of shares of our common stock will have rights, subject to certain conditions, to require us to file registration statements covering their shares or to include their shares in registration statements that we may file for ourselves or other stockholders. We have registered and intend to continue to register all shares of common stock that we may issue under our equity compensation plans. Once we register these shares, they can be freely sold in the public market upon issuance, subject to volume limitations applicable to affiliates and the lock-up agreements described in the “Underwriting” section of this prospectus.
We are an “emerging growth company” and are taking advantage of reduced disclosure and governance requirements applicable to emerging growth companies, which could result in our common stock being less attractive to investors.
We are an “emerging growth company,” as defined in the JOBS Act, and we are taking advantage of certain exemptions from various reporting requirements that are applicable to other public companies that are not emerging growth companies including, but not limited to, not being required to comply with the auditor attestation requirements of Section 404 of the Sarbanes-Oxley Act, reduced disclosure obligations regarding executive compensation in our periodic reports and proxy statements, and exemptions from the requirements of holding a nonbinding advisory vote on executive compensation and stockholder approval of any golden parachute payments not previously approved. We cannot predict if investors will find our common stock less attractive because we will rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile. We may take advantage of these reporting exemptions until we are no longer an emerging growth company, which in certain circumstances could be for up to five years. We will cease to be an “emerging growth company” upon the earliest of: (1) December 31, 2019; (2) the last day of the first fiscal year in which our annual gross revenues are $1 billion or more; (3) the date on which we have, during the previous rolling three-year period, issued more than $1 billion in non-convertible debt securities; and (4) the date on which we are deemed to be a “large accelerated filer” as defined in the Exchange Act.
Our status as an “emerging growth company” under the JOBS Act may make it more difficult to raise capital as and when we need it.
Because of the exemptions from various reporting requirements provided to us as an “emerging growth company” we may be less attractive to investors and it may be difficult for us to raise additional capital as and when we need it. Investors may be unable to compare our business with other companies in our industry if they believe that our financial accounting is not as transparent as other companies in our industry. If we are unable to raise additional capital as and when we need it, our financial condition and results of operations may be materially and adversely affected.
We have incurred and will continue to incur increased costs as a result of being a public company and our management expects to devote substantial time to public company compliance programs.
As a public company, we have incurred and will continue to incur significant legal, accounting and other expenses. We are subject to the reporting requirements of the Exchange Act, which require, among other things, that we file with the SEC annual, quarterly and current reports with respect to our business and financial condition. In addition, the Sarbanes-Oxley Act, as well as rules subsequently adopted by the SEC and The Nasdaq Stock Market to implement provisions of the Sarbanes-Oxley Act, impose significant requirements on public companies, including requiring establishment and maintenance of effective disclosure and financial controls and changes in corporate governance
48
practices. Further, pursuant to the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010, the SEC has adopted and will adopt additional rules and regulations, such as mandatory “say on pay” voting requirements, that will apply to us when we cease to be an emerging growth company. Stockholder activism, the current political environment and the potential for future regulatory reform may lead to substantial new regulations and disclosure obligations, which may lead to additional compliance costs and impact the manner in which we operate our business in ways we cannot currently anticipate.
The rules and regulations applicable to public companies have substantially increased our legal and financial compliance costs and make some activities more time-consuming and costly. To the extent these requirements divert the attention of our management and personnel from other business concerns, they could have a material adverse effect on our business, financial condition and results of operations. The increased costs will decrease our net income or increase our net loss, and may require us to reduce costs in other areas of our business or increase the prices of our products or services. For example, we expect these rules and regulations to make it more difficult and more expensive for us to obtain director and officer liability insurance, and we may be required to incur substantial costs to maintain the same or similar coverage. The impact of these requirements could also make it more difficult for us to attract and retain qualified persons to serve on our board of directors, our board committees or as executive officers.
We previously identified and remediated a material weakness in our internal control over financial reporting. We may identify additional material weaknesses in the future that may cause us to fail to meet our reporting obligations or result in material misstatements of our financial statements. If we fail to remediate any material weaknesses or if we fail to establish and maintain effective control over financial reporting, our ability to accurately and timely report our financial results could be adversely affected.
Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements in accordance with US generally accepted accounting principles. A material weakness is a deficiency, or a combination of deficiencies, in internal control over financial reporting such that there is a reasonable possibility that a material misstatement of annual or interim financial statements will not be prevented or detected on a timely basis.
Prior to the completion of our initial public offering, we were a private company with limited accounting personnel and other resources to address our internal control over financial reporting. During the course of preparing for our initial public offering, we determined that we had a material weakness in our internal control over financial reporting as of December 31, 2013 relating to the design and operation of our closing and financial reporting processes.
While we have remediated this weakness, if we are unable to successfully maintain effective control over financial reporting, and if we are unable to produce accurate and timely financial statements, our stock price may be adversely affected and we may be unable to maintain compliance with applicable listing requirements of The Nasdaq Stock Market.
Because we do not anticipate paying any cash dividends on our capital stock in the foreseeable future, capital appreciation, if any, will be your sole source of potential gain.
We have never declared or paid cash dividends on our capital stock. We currently intend to retain all of our future earnings, if any, to finance the growth and development of our business. In addition, the terms of any future debt agreements may preclude us from paying dividends. As a result, capital appreciation, if any, of our common stock will be your sole source of gain for the foreseeable future.
49
Future sales and issuances of our common stock or rights to purchase common stock, including pursuant to our equity incentive plans, could result in additional dilution of the percentage ownership of our stockholders and could cause our stock price to fall.
We expect that significant additional capital will be needed in the future to continue our planned operations. To raise capital, we may sell substantial amounts of common stock or securities convertible into or exchangeable for common stock. These future issuances of common stock or common stock-related securities, together with the exercise of outstanding options and any additional shares issued in connection with acquisitions or in-licenses, if any, may result in material dilution to our investors. Such sales may also result in material dilution to our existing stockholders, and new investors could gain rights, preferences and privileges senior to those of holders of our common stock, including the shares of common stock sold in this offering.
Pursuant to our equity incentive plans, our compensation committee is authorized to grant equity-based incentive awards to our employees, non-employee directors and consultants. Future grants of RSUs, options and other equity awards and issuances of common stock under our equity incentive plans will result in dilution and may have an adverse effect on the market price of our common stock.
We have broad discretion in the use of the net proceeds from this offering and may not use them effectively.
Although we currently intend to use the net proceeds from this offering and our other capital resources in the manner described in “Use of Proceeds” elsewhere in this prospectus, our management will have broad discretion in the application of the net proceeds from this offering and could spend the proceeds in ways that do not improve our results of operations or enhance the value of our common stock. The failure by our management to apply these funds effectively could result in financial losses that could have a material adverse effect on our business, cause the market price of our common stock to decline and delay the development of our product candidates. Pending their use, we may invest the net proceeds from this offering in a manner that does not produce income or that loses value. If we do not invest the net proceeds from this offering in ways that enhance stockholder value, we may fail to achieve expected financial results, which could cause the price of our common stock to decline.
Some provisions of our charter documents and Delaware law may have anti-takeover effects that could discourage an acquisition of us by others, even if an acquisition would be beneficial to our stockholders and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our amended and restated certificate of incorporation, or certificate of incorporation, and amended and restated bylaws, or bylaws, as well as provisions of Delaware law, could make it more difficult for a third party to acquire us or increase the cost of acquiring us, even if doing so would benefit our stockholders, or remove our current management. These include provisions that will:
| • | permit our board of directors to issue up to 20,000,000 shares of preferred stock, with any rights, preferences and privileges as they may designate; |
| • | provide that all vacancies on our board of directors, including as a result of newly created directorships, may, except as otherwise required by law, be filled by the affirmative vote of a majority of directors then in office, even if less than a quorum; |
| • | require that any action to be taken by our stockholders must be effected at a duly called annual or special meeting of stockholders and not be taken by written consent; |
50
| • | provide that stockholders seeking to present proposals before a meeting of stockholders or to nominate candidates for election as directors at a meeting of stockholders must provide advance notice in writing, and also specify requirements as to the form and content of a stockholder’s notice; |
| • | not provide for cumulative voting rights, thereby allowing the holders of a majority of the shares of common stock entitled to vote in any election of directors to elect all of the directors standing for election; and |
| • | provide that special meetings of our stockholders may be called only by the board of directors or by such person or persons requested by a majority of the board of directors to call such meetings. |
These provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors, who are responsible for appointing the members of our management. Because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which may discourage, delay or prevent someone from acquiring us or merging with us whether or not it is desired by or beneficial to our stockholders. Under Delaware law, a corporation may not, in general, engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other things, the board of directors has approved the transaction. Any provision of our amended and restated certificate of incorporation or amended and restated bylaws or Delaware law that has the effect of delaying or deterring a change in control could limit the opportunity for our stockholders to receive a premium for their shares of our common stock, and could also affect the price that some investors are willing to pay for our common stock.
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our stock price and trading volume could decline.
The trading market for our common stock will depend in part on the research and reports that securities or industry analysts publish about us or our business. In the event securities or industry analysts who cover us downgrade our stock or publish inaccurate or unfavorable research about our business, our stock price would likely decline. If one or more of these analysts cease coverage of our company or fail to publish reports on us regularly, demand for our stock could decrease, which might cause our stock price and trading volume to decline.
51
SPECIAL NOTE REGARDING FORWARD-LOOKING STATEMENTS AND INDUSTRY DATA
This prospectus and the documents incorporated by reference contain forward-looking statements. The forward-looking statements are contained principally in the sections titled “Prospectus Summary,” “Risk Factors,” “Use of Proceeds,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “Business” in this prospectus or the documents incorporated by reference. In some cases you can identify these statements by forward-looking words such as “believe,” “may,” “will,” “estimate,” “continue,” “anticipate,” “intend,” “could,” “would,” “project,” “plan,” “expect” or the negative or plural of these words or similar expressions. These forward-looking statements include, but are not limited to, statements concerning the following:
| • | our expectations regarding the timing of reporting results from our Phase 2 clinical trials of PINTA 745, EBV-CTL and CMV-CTL; |
| • | our expectations regarding the timing of reporting results from our Phase 1 clinical studies of STM 434 and WT1-CTL; |
| • | the likelihood and timing of regulatory approvals for our product candidates; |
| • | the potential market opportunities for commercializing our product candidates; |
| • | our expectations regarding the potential market size and the size of the patient populations for our product candidates, if approved for commercial use; |
| • | estimates of our expenses, capital requirements and need for additional financing; |
| • | our expectation that our existing capital resources and net proceeds from this offering will be sufficient to enable us to complete our planned confirmatory Phase 2 clinical trial of PINTA 745, our initial Phase 1 clinical study of STM 434, the ongoing and planned studies and trials with our T-cell product candidates, and fund our operations and capital expenditure requirements into the second half of 2018; |
| • | our ability to develop, acquire and advance product candidates into, and successfully complete, clinical studies and trials; |
| • | the initiation, timing, progress and results of future preclinical studies and clinical trials and our research and development programs; |
| • | the scope of protection we are able to obtain and maintain for our intellectual property rights covering our product candidates; |
| • | our use of proceeds from this offering; |
| • | our financial performance; |
| • | developments and projections relating to our competitors and our industry; and |
| • | our ability to sell or manufacture products at commercially reasonable values. |
These statements are only current predictions and are subject to known and unknown risks, uncertainties and other factors that may cause our or our industry’s actual results, levels of activity, performance or achievements to be materially different from those anticipated by the forward-looking statements. We discuss many of these risks in this prospectus in greater detail under the heading “Risk Factors” and elsewhere in this prospectus and the documents incorporated by reference. You should not rely upon forward-looking statements as predictions of future events. New risk factors and uncertainties may emerge from time to time, and it is not possible for management to predict all risks and uncertainties.
Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee future results, levels of activity, performance or achievements.
52
Except as required by law, after the date of this prospectus, we are under no duty to update or revise any of the forward-looking statements, whether as a result of new information, future events or otherwise.
We obtained industry, market and competitive position data in this prospectus from our own internal estimates and research as well as from industry and general publications and research surveys and studies conducted by third parties. These data involve a number of assumptions and limitations, and you are cautioned not to give undue weight to such information or estimates.
53
We estimate that we will receive net proceeds from the sale of shares of common stock in this offering of approximately $ million after deducting underwriting discounts and commissions and estimated offering expenses, based on an assumed public offering price of $ per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on , 2015. If the underwriters’ option to purchase additional shares of common stock is exercised in full, we estimate that we will receive net proceeds of approximately $ million after deducting underwriting discounts and commissions and estimated offering expenses, based on an assumed public offering price of $ per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on , 2015.
As of March 31, 2015, we had cash and cash equivalents and short-term investments of $166.7 million. We currently estimate that we will use the net proceeds from this offering, together with our existing cash and cash equivalents and short-term investments, as follows:
| • | approximately $43 million for clinical development and related manufacturing for PINTA 745, including the cost of our ongoing Phase 2 clinical trial and our planned confirmatory Phase 2 clinical trial expected to take place thereafter, together with potential additional trials in other indications; |
| • | approximately $25 million to fund the clinical development and related manufacturing of STM 434, including the cost of our ongoing Phase 1 clinical study and possible expansion of our current Phase 1 clinical trial for STM 434 to include other solid tumors; |
| • | approximately $72 million for ongoing and future clinical studies with our current T-cell product candidates licensed from MSK including additional studies with EBV-CTL in EBV-LPD and additional studies with CMV-CTL in refractory CMV infection as well as related manufacturing, sponsored research in collaboration with MSK and other required payments to MSK; and |
| • | the remainder to continue to expand and advance our clinical and preclinical pipeline and for working capital and for other general corporate purposes and to potentially acquire or license other product candidates, businesses or technologies, although we have no present commitments for any such acquisitions or licenses. |
This expected use of our net proceeds from this offering and other capital resources represents our intentions based upon our current plans and business conditions, which could change in the future as our plans and business conditions evolve. The amounts and timing of our actual expenditures may vary significantly depending on numerous factors, including the progress of our development, the status of and results from preclinical and clinical trials, as well as any collaborations that we may enter into with third parties for our product candidates, and any unforeseen cash needs. As a result, our management will retain broad discretion over the allocation of the net proceeds of this offering.
Based on our planned use of capital resources described above, we estimate that the net proceeds from this offering, together with our existing cash and cash equivalents and short-term investments, will enable us to complete our planned confirmatory Phase 2 clinical trial of PINTA 745, our initial Phase 1 clinical study of STM 434, the ongoing and planned studies and trials with our T-cell product candidates, and fund our operations and capital expenditure requirements into the second half of 2018. Pending our use of our net proceeds from this offering, we intend to invest the net proceeds in a variety of capital preservation investments, including short-term, investment-grade, interest-bearing instruments and US government securities.
54
MARKET PRICE OF OUR COMMON STOCK
Our common stock is listed on The Nasdaq Global Select Market under the symbol “ATRA” since October 16, 2014. Prior to that date, there was no public trading market for our common stock. The following table sets forth for the periods indicated the high and low sales prices per share of our common stock as reported on The Nasdaq Global Select Market:
| High | Low | |||||||
| Year ended December 31, 2014 |
||||||||
| Fourth Quarter (from October 16, 2014) |
$ | 35.45 | $ | 9.66 | ||||
| Year ending December 31, 2015 |
||||||||
| First Quarter |
$ | 43.66 | $ | 17.20 | ||||
| Second Quarter (through June 26, 2015) |
$ | 64.35 | $ | 36.00 | ||||
On June 26, 2015, the last reported sale price of our common stock on The Nasdaq Global Select Market was $52.62 per share. As of May 31, 2015, we had 17 holders of record of our common stock. The actual number of stockholders is greater than this number of record holders, and includes stockholders who are beneficial owners, but whose names are held in street name by brokers and other nominees. This number of holders of record also does not include stockholders whose shares may be held in trust by other entities.
55
We do not anticipate declaring or paying any cash dividends on our capital stock. Any future determination as to the declaration and payment of dividends, if any, will be at the discretion of our board of directors and will depend on then existing conditions, including our financial condition, operating results, contractual restrictions, capital requirements, business prospects and other factors our board of directors may deem relevant.
56
The following table sets forth our cash and cash equivalents, short-term available-for-sale investments and our capitalization as of March 31, 2015:
| • | on an actual basis; and |
| • | on an as adjusted basis to reflect the sale of shares of common stock in this offering at an assumed public offering price of $ per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on , 2015, after deducting underwriting discounts and commissions and estimated offering expenses. |
You should read the information in this table together with our consolidated and combined financial statements and related notes appearing in our 2014 Annual Report and our March 2015 Quarterly Report, as well as the information in the sections titled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” appearing in our 2014 Annual Report and our March 2015 Quarterly Report incorporated by reference herein.
| As of March 31, 2015 | ||||||||
| Actual | As Adjusted | |||||||
| (in thousands, except share data) | ||||||||
| (unaudited) | ||||||||
| Cash and investments: |
||||||||
| Cash and cash equivalents |
$ | 71,329 | $ | |||||
| Short-term available-for-sale investments |
95,367 | |||||||
|
|
|
|
|
|||||
| $ | 166,696 | $ | ||||||
|
|
|
|
|
|||||
| Stockholders’ equity: |
||||||||
| Common stock—$0.0001 par value, 23,911,930 shares issued and outstanding, actual; shares issued and outstanding, as adjusted |
2 | |||||||
| Additional paid-in capital |
216,159 | |||||||
| Accumulated other comprehensive loss |
(18 | ) | ||||||
| Accumulated deficit |
(50,049 | ) | ||||||
|
|
|
|
|
|||||
| Total stockholders’ equity |
166,094 | |||||||
|
|
|
|
|
|||||
| Total capitalization |
$ | 166,094 | $ | |||||
|
|
|
|
|
|||||
The as adjusted outstanding share information in the table above is based on 23,911,930 shares of our common stock outstanding as of March 31, 2015, and excludes the following:
| • | 906,391 shares of common stock issuable upon settlement of RSUs outstanding as of March 31, 2015; |
| • | 1,314,635 shares of common stock issuable upon the exercise of options outstanding as of March 31, 2015 with an exercise price of $19.61 per share; |
| • | 448,317 shares of restricted stock that remained subject to vesting as of March 31, 2015; |
| • | 2,046,541 shares of common stock reserved for future issuance under our 2014 Plan as of March 31, 2015; |
| • | 432,898 shares of common stock reserved for issuance under our ESPP as of March 31, 2015; and |
| • | any future automatic increases in the number of shares of common stock reserved for issuance under our 2014 Plan or ESPP. |
57
If you invest in our common stock, your interest will be diluted to the extent of the difference between the public offering price per share of our common stock and the as adjusted net tangible book value per share of our common stock immediately after this offering.
Our historical net tangible book value as of March 31, 2015 was approximately $166.1 million, or $6.95 per share of common stock. Our historical net tangible book value is the amount of our total tangible assets less our liabilities. Historical net tangible book value per share is our historical net tangible book value divided by 23,911,930, the number of shares of common stock outstanding as of March 31, 2015.
After giving effect to our receipt of the net proceeds from our sale of shares of our common stock in this offering at an assumed public offering price of $ per share, the last reported sale price of our common stock on The Nasdaq Global Select Market on , 2015, after deducting underwriting discounts and commissions and estimated offering expenses, our as adjusted net tangible book value as of March 31, 2015 would have been approximately $ million, or $ per share. This represents an immediate increase in as adjusted net tangible book value of $ per share to our existing stockholders and an immediate dilution of $ per share to investors purchasing common stock in this offering.
The following table illustrates this dilution on a per share basis to new investors:
| Assumed public offering price per share |
$ | |||||||
| Historical net tangible book value per share as of March 31, 2015 |
$ | 6.95 | ||||||
| Increase in net tangible book value attributable to new investors |
||||||||
|
|
|
|||||||
| As adjusted net tangible book value per share after this offering |
||||||||
|
|
|
|||||||
| Dilution per share to investors participating in this offering |
$ | |||||||
|
|
|
The number of shares of common stock to be outstanding after this offering is based on 23,911,930 shares of our common stock outstanding as of March 31, 2015 and assumes the issuance and sale of shares of our common stock in this offering at an assumed public offering price of $ per share, the last reported sale price of our common stock on the Nasdaq Global Select Market on , 2015, and excludes the following:
| • | 906,391 shares of common stock issuable upon settlement of restricted stock units, or RSUs, outstanding as of March 31, 2015; |
| • | 1,314,635 shares of common stock issuable upon the exercise of options outstanding as of March 31, 2015 with an exercise price of $19.61 per share; |
| • | 448,317 shares of restricted stock that remained subject to vesting as of March 31, 2015; |
| • | 2,046,541 shares of common stock reserved for future issuance under our 2014 Equity Incentive Plan, or 2014 Plan as of March 31, 2015; |
| • | 432,898 shares of common stock reserved for issuance under our 2014 Employee Stock Purchase Plan, or our ESPP, as of March 31, 2015; and |
| • | any future automatic increases in the number of shares of common stock reserved for issuance under our 2014 Plan or our ESPP. |
58
Overview
We are a clinical-stage biopharmaceutical company focused on developing novel therapeutics for serious unmet medical needs, with an initial focus on muscle wasting conditions, oncology, and viral-associated diseases. We have two groups of product candidates: molecularly targeted biologics and allogeneic, or third-party derived, antigen-specific T-cells, a type of white blood cell. Our molecularly targeted product candidates are biologics that inhibit myostatin and activin, members of the Transforming Growth Factor-Beta, or TGF-ß, protein superfamily, which play roles in the growth and maintenance of muscle and many other body tissues. Our lead molecularly targeted product candidate, PINTA 745, is in a Phase 2 clinical trial for protein energy wasting, or PEW, a condition affecting many end-stage renal disease, or ESRD patients. Our second molecularly targeted product candidate is STM 434. We commenced a Phase 1 clinical study of STM 434 for ovarian cancer and other solid tumors in 2014. We have five additional molecularly targeted product candidates that modulate the TGF-ß pathway in preclinical development. Our T-cell product candidates arise from a platform technology designed to produce off-the-shelf, partially human leukocyte antigen, or HLA, matched cellular therapeutics. We licensed rights to these product candidates from Memorial Sloan Kettering Cancer Center, or MSK, in June 2015. Our initial T-cell product candidates target viral- or cancer-specific antigens and are designed to harness the body’s immune system to counteract specific viral infections and cancers. Our most advanced T-cell product candidate, EBV-CTL, is in Phase 2 clinical trials for malignancies associated with Epstein-Barr Virus, including EBV-associated lymphoproliferative diseases, or EBV-LPD. EBV-LPD is a cancer affecting some patients who have received an allogeneic hematopoietic cell transplant, or HCT, a solid organ transplant, or SOT, or are otherwise immunocompromised. In February 2015, the US Food and Drug Administration, or the FDA, granted Breakthrough Therapy designation for EBV-CTL in the treatment of rituximab-refractory EBV-LPD after HCT. Our second T-cell product candidate, CMV-CTL, is in Phase 2 clinical trials for cytomegalovirus, or CMV, an infection that occurs in some patients who have received an HCT or SOT or are otherwise immunocompromised. Our third T-cell product candidate, WT1-CTL, targets cancers expressing the antigen Wilms Tumor 1, or WT1, and is currently in Phase 1 clinical studies. In addition, we have entered into a sponsored research collaboration with MSK to discover and develop additional T-cell product candidates, including chimeric antigen receptor modified T-cells, or CAR-T cells.
Our lead molecularly targeted product candidate, PINTA 745, is a peptibody that binds to and inhibits myostatin, a protein that downregulates muscle growth and maintenance. In a Phase 1 study, PINTA 745 was found to increase muscle mass compared to placebo after one month of weekly dosing, an increase that was statistically significant, indicating that it is more likely than not that the benefit observed in the study was due to drug treatment rather than chance. We are enrolling a US-based Phase 2 clinical trial to further establish the role of PINTA 745 in building muscle mass, as well as to collect data from corresponding functional muscle tests. This trial is being conducted in patients with ESRD who are also suffering from PEW, a condition characterized by muscle wasting, inflammation and malnutrition.
PEW is a major complication of ESRD. A recent study we completed with DaVita Clinical Research, a division of DaVita Healthcare Partners Inc., concluded that more than half of the patients in DaVita’s dialysis population meet the conditions for PEW and, in comparison to the rest of the group, exhibit worse morbidity and mortality. There is currently no approved therapy for patients suffering from PEW. We believe PINTA 745 is the only therapeutic in clinical development to treat this patient population.
59
In clinical studies conducted of PINTA 745 in men with prostate cancer and in mouse studies in a model of chronic kidney disease, or CKD, conducted with PINTA 745/s, a version of PINTA 745 that was customized for use in mice, several properties well suited for a potential therapeutic for PEW were observed, including:
| • | Reversing muscle loss — PINTA 745 not only stopped muscle wasting, it significantly increased muscle mass after four weeks of treatment. |
| • | Anti-inflammatory properties — In an animal model of renal disease, PINTA 745/s exhibited significant anti-inflammatory properties, a factor that we believe will be important due to the critical role that inflammation plays in PEW and the overall declining health of ESRD patients. |
| • | Dosing schedule — PINTA 745 is dosed weekly, which conveniently aligns with dialysis treatment schedules. |
We designed the Phase 2 trial to give us insight into potential additional therapeutic areas for PINTA 745. These could include: orthopedic indications; inflammation and inflammatory diseases; age-related sarcopenia, or loss of muscle; and cancer cachexia, a syndrome of progressive weight loss. In each of these conditions, muscle loss prevention, muscle growth and reduction in inflammation resulting from treatment with PINTA 745 could lead to improved physical function and therefore to better outcomes. As of June 30, 2015, we had enrolled of the planned 48 patients, and we expect to release preliminary data from this Phase 2 clinical trial in the fourth quarter of 2015 and to present data at a major scientific meeting in 2016.
Our second molecularly targeted product candidate, STM 434, is in a Phase 1 clinical study that will enroll approximately 66 patients with ovarian cancer and other solid tumors. STM 434 is a soluble ActR2B receptor that binds Activin A. Activin has been shown to be involved in the growth and proliferation of ovarian cancer and other tumors, with published evidence of its role at both the genetic (messenger RNA) and protein levels. Activin expression is one of a few biomarkers associated with larger tumor volume and poorer outcomes, including shortened survival, in a variety of tumors including ovarian tumors. Published data has shown that serum Activin A levels in ovarian cancer subjects are elevated in relation to levels in normal subjects. We are testing the potential use of Activin A as a biomarker in our Phase 1 clinical study.
Ovarian cancer is the fifth leading cause of cancer death in women in the United States. Surgery and cytotoxic chemotherapies are widely used to treat ovarian cancer; however, the outcomes have changed little in 40 years. The proportion of all ovarian cancer patients surviving five years after diagnosis was only 44% based on the National Cancer Institute SEER database for women diagnosed from 2003 to 2009.
Some subtypes of ovarian tumors respond even more poorly to treatment than others and represent opportunities where drug development could be accelerated. In particular, clear cell and granulosa cell tumors are considered resistant to chemotherapy. Our preclinical experiments in animal models of these subtypes indicate that binding Activin A with a soluble receptor could significantly reduce tumor proliferation, reduce tumor volume and potentially increase survival. We believe that novel therapies for clear cell and granulosa cell tumors could qualify for Breakthrough Therapy designation, an FDA process designed to accelerate the development and review of drugs intended to treat a serious condition when early studies show that the drug may be substantially better than current treatment. Based on its mechanism of action, we also believe that STM 434 has the potential to be the first product to target tumor growth and proliferation through the inhibition of Activin A.
Both PINTA 745 and STM 434 are novel molecules with well-characterized mechanisms of action. They were developed initially, along with our five other in-licensed molecularly targeted biologic
60
programs, at Amgen. Taken together, we believe these product candidates constitute a pipeline of biologics that have benefited from years of investment, resulting in a large patent portfolio, broad preclinical testing and, in the case of PINTA 745, promising clinical results. We are evaluating the remaining five molecularly targeted product candidates to determine the best path forward. Where appropriate, we intend to conduct preclinical studies and file investigational new drug applications, or INDs, with the FDA for these candidates. For example, we are conducting IND-enabling manufacturing and preclinical studies for ATA 842, a humanized antibody targeting myostatin.
Our two most advanced T-cell product candidates, EBV-CTL and CMV-CTL, target viral antigens from EBV and CMV, respectively. These viruses are associated with various types of cancer, severe infections and certain neurologic conditions that lead to a high degree of morbidity and mortality in some patients. These T-cell product candidates are intended to work by targeting the abnormal cells expressing the applicable target antigen and killing them. Both product candidates are in ongoing Phase 2 clinical trials with published proof of concept data in highly refractory, difficult to treat patient populations. We believe that the clinical data generated to date with EBV-CTL in the post-HCT and post-SOT settings and with CMV-CTL in the post-HCT setting may support a rapid path to marketing approvals in these rare conditions if supported by additional clinical data. Furthermore, we believe that EBV-CTL and CMV-CTL have the potential to be the first targeted allogeneic cellular therapies approved for the treatment of cancer and persistent viral infections.
In clinical studies that enrolled patients with EBV-LPD following HCT or SOT, efficacy following treatment with EBV-CTL compares favorably with historical data in these patient populations. In rituximab-refractory patients with EBV-LPD after HCT, treatment with EBV-CTL resulted in two-year overall survival ranging from 46.9 to 63.8% in two separate clinical trials in comparison with historical data suggesting an expected median survival, or the time by which 50% of patients are expected to have died, of 16-56 days. In the setting of rituximab refractory EBV-LPD after SOT, similar results were observed, with two-year overall survival of 57.7% in EBV-CTL-treated patients in comparison with an expected historical 2-year survival ranging from 0 to 33%. In February 2015, the FDA granted Breakthrough Therapy designation for EBV-CTL in the treatment of rituximab refractory EBV-LPD after HCT. We recently met with the FDA to discuss late-stage development to support a potential approval in this indication. Based on guidance from the FDA, we intend to conduct a pivotal study in rituximab-refractory EBV-LPD after HCT and expect to submit a special protocol assessment for this pivotal study. In addition, we had preliminary discussions with the FDA regarding late-stage development in the setting of rituximab-refractory EBV-LPD after SOT, and we will be incorporating this feedback into our subsequent development plans in this indication. Results from ongoing Phase 2 studies of CMV-CTL have demonstrated similar efficacy in the setting of refractory CMV infection after HCT, with response rates exceeding 60% in patients with CMV viremia and disease resistant to multiple approved and investigational anti-viral therapies.
While we evaluate the path to registration for both EBV-CTL and CMV-CTL in these initial indications, we intend to concurrently explore the clinical utility of these T-cell product candidates or other cellular therapies in other relevant disease states to expand their potential applicability. In addition, we believe that T-cells can be directed at a broad range of other targets to create future product candidates. As a result we intend to develop novel cellular therapies against other antigens of interest including, for example, human papilloma virus, or HPV, John Cunningham virus, or JCV, as well as other cancer and viral-associated targets. We believe that viral antigens are well suited to adoptive immunotherapy given that people with normal immune systems are able to mount robust responses to these viral targets, but immunocompromised patients and some cancer patients are not.
Our business model is to license or acquire and develop novel therapeutics for serious unmet medical needs with validated targets and established proof of concept. Based on the properties of each of these molecules, including efficacy, safety, pharmacokinetics, affinity and other characteristics, we match each program to clinical indications that we believe maximize its therapeutic potential and may
61
result in an expedited path to market. We believe our management team has the breadth and depth of experience to execute this model. Our management team includes:
| • | Isaac E. Ciechanover, M.D., our President and Chief Executive Officer, was Executive Director for Business Development at Celgene. At Celgene, he led the company’s venture capital efforts and led licensing and acquisition activities with an aggregate transaction value of more than $6.7 billion. Those efforts included striking licensing and partnership transactions with cancer therapeutics companies Agios Pharmaceuticals, Inc., Acceleron Pharma Inc. and PTC Therapeutics Inc. Prior to founding Atara, Dr. Ciechanover was a Partner with Kleiner Perkins Caufield & Byers, a leading venture capital firm. |
| • | Christopher Haqq, M.D., Ph.D., our Chief Medical Officer, was Vice President for Clinical Research and Development at Cougar Biotechnology, which was acquired by Johnson & Johnson in 2009. At Cougar Biotechnology, he was the lead clinician for a pivotal prostate cancer study leading to market approval for Zytiga (abiraterone acetate). He has served as medical monitor for more than ten clinical trials and has contributed to drug development programs for a wide range of molecules, and served as an attending oncology physician and director of a translational laboratory at the University of California, San Francisco. |
| • | Mitchall G. Clark, our Chief Regulatory and Quality Officer, was previously Senior Vice President of Global Regulatory Affairs at Abraxis Bioscience, Inc., or Abraxis, where he submitted and managed five INDs for oncology and cardiovascular drugs including Abraxane (nanoparticle albumin-bound paclitaxel). |
| • | Gad Soffer, our Chief Operating Officer, previously held various roles at Celgene, including most recently Global Project Leader for Abraxane following Celgene’s acquisition of Abraxis, where he led successful regulatory submissions for pancreatic cancer and non-small cell lung cancer. |
| • | John F. McGrath, Jr., our Chief Financial Officer, was previously Executive in Residence and Operating Partner at Kleiner Perkins Caufield & Byers. Prior to that time, he served as Vice President and Chief Financial Officer for Network Equipment Technologies, Inc., a publicly traded company. He has served on the board of directors of the Presidio Fund, a publicly traded mutual fund, and on the boards of directors and as Audit Committee chairman of publicly traded companies Actel Corporation and Endwave Corporation. |
Our Strategy
Our goal is to be a leader in the development and commercialization of novel therapeutics for serious unmet medical needs. We are initially focused on muscle wasting conditions, oncology, and infectious disease. Key components of our strategy to achieve this objective include:
| • | Rapidly advance PINTA 745 in clinical development — We intend to complete our ongoing Phase 2 clinical trial of PINTA 745 with the goal of obtaining positive results in ESRD patients with PEW. If the data supports it, we intend to seek feedback from health authorities, including the FDA, and advance PINTA 745 to global registration trials in PEW. In parallel, we intend to seek out additional indications for which to explore the therapeutic utility of PINTA 745. |
| • | Obtain clinical proof of concept for STM 434 — In 2014, we commenced a Phase 1 study of STM 434 to study safety and tolerability as well as early signs of activity in a patient population that includes patients with ovarian cancer and other solid tumors. We intend to test STM 434 as a single therapy and in combination with other chemotherapy options that are the current standard of care. In the clear cell and granulosa cell subtypes of ovarian cancer, we may seek orphan drug status. If supported by the clinical data, we may pursue clinical trials with STM 434 in these specific subtypes and seek Breakthrough Therapy designation. |
62
| • | Evaluate our other molecularly targeted product candidates and advance them into the clinic as appropriate — Our initial product portfolio includes five additional unique molecularly targeted product candidates that have not yet entered clinical trials. We will evaluate these product candidates and determine which of them to advance and the indications in which to develop them. |
| • | Rapidly advance EBV-CTL in clinical development for the treatment of EBV-LPD after HCT or SOT — We intend to continue our ongoing Phase 2 clinical trials of EBV-CTL and execute on a plan discussed with the FDA and other health authorities for late-phase development to support potential marketing approvals in rituximab refractory EBV-LPD after HCT, the indication for which Breakthrough Therapy designation was granted in February 2015. In addition, we intend to proceed with late-phase development to support potential marketing approvals in rituximab-refractory EBV-LPD after SOT and explore the therapeutic utility of EBV-CTL in other relevant disease states. We may also seek orphan drug status, where appropriate. |
| • | Develop CMV-CTL based on existing clinical proof of concept data in refractory CMV infection after HCT — We intend to continue to support the ongoing Phase 2 clinical studies of CMV-CTL and meet with health authorities to establish a plan for late-phase development to support potential marketing approvals in treatment of anti-viral resistant CMV viremia and symptomatic disease, including retinitis. In parallel, we intend to explore the therapeutic utility of CMV-CTL in other relevant indications. We may also seek orphan drug status, where appropriate. |
| • | Continue development of WT1-CTL and collaborate with MSK in the discovery and development of additional T-cell programs — We intend to continue to support the ongoing Phase 1 clinical trials of WT1-CTL in acute myeloid leukemia, or AML, and multiple myeloma and, if supported by the clinical data, expand clinical development in hematologic malignancies. In parallel, we intend to collaborate with MSK on the development of other T-cell programs by utilizing the existing technology platform to target other antigens and research on other cellular therapy modalities. |
| • | Leverage our relationships and experience to in-license or acquire additional product candidates or technologies for development — We intend to continue to capitalize on our relationships with both pharmaceutical companies and academic institutions to identify, review and ultimately license or acquire novel product candidates for development or collaborate with others to enhance our ability to develop and commercialize our existing product candidates. |
Our Molecularly Targeted Product Candidates
PINTA 745 for Protein-Energy Wasting in End-Stage Renal Disease Patients
Our lead molecularly targeted product candidate, PINTA 745, is a peptibody that binds myostatin and inhibits its corresponding signal transduction, thereby blocking the negative regulation of skeletal muscle growth. We are conducting a Phase 2 trial in patients with ESRD who are also suffering from PEW at six US-based sites, including academic sites, as well as those associated with Fresenius and DaVita, two leading providers of kidney care in the United States. PEW refers to a state of muscle wasting, inflammation and malnutrition that increases patients’ risk for infections, cardiovascular disease and other complications. We believe that patients with PEW may benefit from the muscle-building demonstrated in earlier clinical trials and anti-inflammatory properties of PINTA 745 demonstrated in preclinical trials, which are discussed in more detail below. INDs for PINTA 745 were filed by Amgen, the product candidate’s previous sponsor, in October 2005 and July 2009. Both of these INDs are open, with our wholly owned subsidiary Pinta as the holder.
63
Protein-Energy Wasting in ESRD Patients
PEW is a common and serious condition affecting patients on kidney dialysis. Patients with PEW lose significant body mass and suffer from muscle wasting and weakness. In several published studies, PEW has been shown to increase the already high morbidity and mortality associated with ESRD. A study published in 2010 examined 40,950 dialysis patients from 12 countries and showed that PEW increases patients’ risk for infections, cardiovascular disease and other complications. Another study published in 2010 examined more than 120,000 dialysis patients and found that patients who lost overall body weight but gained muscle mass had a higher survival rate.
Many dialysis patients with PEW experience a lower quality of life due to poor limb strength, low endurance and impaired muscle power. Worsening of walking speed and grip strength, associated with loss of muscle mass, have been shown to be effective predictors of mortality.
Albumin is the most abundant protein circulating in the blood and a sensitive indicator of the body’s nutritional status. In dialysis patients, a decline in serum albumin indicates a serious overall protein wasting state. In these patients, the presence of muscle wasting or inflammation is associated with increased risk of mortality.
DaVita Study
In order to better understand the market opportunity for PEW therapies in dialysis patients, we collaborated on a study of PEW in dialysis patients with DaVita. DaVita has collected data on over 130,000 renal patients including those enrolled in over 300 clinical trials worldwide in order to better understand the pathology and clinical course of kidney disease. The resulting database is a unique and powerful resource that allows for fast understanding of the disease state and the impact of treatments in kidney disease.
Using the DaVita dialysis database, we were able to characterize patients for the PEW condition and identify those patients at higher risk of morbidity and mortality. We analyzed 56,350 DaVita dialysis patients who began treatment at DaVita between 2009 and 2012 and had at least six months of dialysis. We then followed these patients from the time they entered the database for 1,200 days or until they died or were lost to follow-up. Of these patients, 54% had a serum albumin level less than or equal to 3.8 g/dL six months after beginning dialysis. Among these, approximately 11% of patients died within one year compared to less than 3% of patients whose serum albumin was higher than the 3.8 g/dL dialysis threshold. At the three-year mark, approximately 40% of patients with low serum albumin who had been followed for three years had died in comparison with roughly 21% of patients who had been followed for three years with serum albumin levels above the critical threshold six months after beginning dialysis. We believe that patients with PEW represent a significant cost to the healthcare system. We and DaVita are currently pursuing health economic studies in order to quantify this cost, comparing treatment for those who have PEW to those who do not.
64
Survival Rates Based Upon Serum Albumin Levels
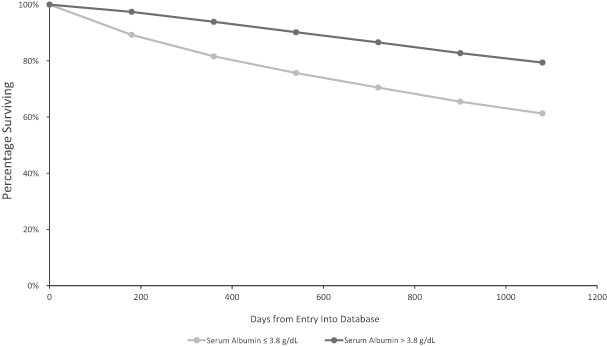
PEW Market Opportunity
Based on data from the US Renal Data System, we estimate that the current total US dialysis population, excluding patients who had successfully received kidney transplants, is 460,000 patients. Of these patients, we estimate that approximately 250,000 patients suffer from PEW. Worldwide, we believe that more than 800,000 patients suffer from PEW.
Limitations of Current Therapies for PEW
There are no pharmacologic therapies approved by the FDA that are indicated for PEW. Furthermore, we are not aware of any such therapies in clinical trials for PEW that target myostatin. Current treatment options for muscle wasting include appetite stimulants, nutritional support, corticosteroids, anabolic steroids and human growth hormone. Dietary supplements containing 10 grams of protein or more per day are recommended for PEW patients by consensus guidelines. Long term stabilization of lean body mass, muscle mass or serum albumin levels in patients showing symptoms of PEW or related conditions such as cancer cachexia have not been observed through dietary changes or nutritional supplements.
Biology of Myostatin
Myostatin, a member of the TGF-ß superfamily of growth factors, is highly expressed in skeletal muscle and fat tissue. It acts as a negative regulator of muscle growth and appears to promote fat gain. Through knockout experiments and observation of naturally occurring knockouts of myostatin in mice, cattle, dogs, as well as a human being, there is a body of evidence supporting the role of myostatin in regulating muscle growth. In particular, myostatin has been shown to inhibit the growth of new muscle stem cells as well as play a part in the destruction of muscle through the NF-KB pathway. Animals and humans born without a functioning myostatin gene exhibit muscle overgrowth while otherwise showing no apparent negative effects.
65
Myostatin inhibition was first characterized and evaluated in the mid-1990s as a potential mechanism for limiting muscle wasting. Several proof-of-concept studies have shown the ability of myostatin inhibitors to build muscle. Several other companies are pursuing myostatin inhibitors for other conditions, including cancer cachexia, Duchenne Muscular Dystrophy and orthopedic indications.
Preclinical studies have shown that myostatin is upregulated, or increased, in the skeletal muscle of mice suffering from chronic kidney disease, or CKD. One such study, published in the FASEB Journal in 2011, is shown below.
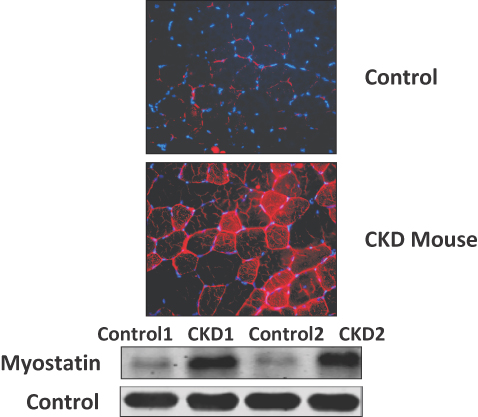
In the two upper images, myostatin upregulation is shown by fluorescence in the muscle cells of a CKD mouse compared to a control mouse. In the two lower images, myostatin protein expression levels are shown in the muscle cells of two CKD mice compared to control mice.
66
The following charts and images from a study published in Kidney International in 2011 show that myostatin is upregulated in skeletal muscle taken from dialysis patients. This was observed both quantitatively and when a thin slice of muscle tissue was examined under a microscope, or histologically.
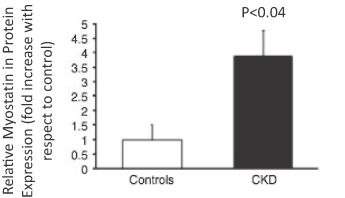
The p-value is a measure of the likelihood that the data observed are from chance instead of due to the effects of the drug tested. The smaller the p-value, the stronger the likelihood that the data observed resulted from the drug tested rather than from chance. By convention, p-values less than 0.05 are considered significant, indicating a high degree of confidence that the result is due to therapy with the drug and not to chance.
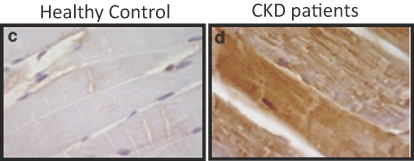
In the upper graphs, myostatin RNA and protein levels are increased in CKD patients compared to healthy controls. In the lower images, myostatin in muscle stains dark in CKD patients compared to healthy controls.
Mechanism of PINTA 745
PINTA 745 is a peptibody, a peptide-antibody combination. The peptide component binds to myostatin, preventing it from docking with its receptors on the surface of muscle cells and blocking its role in inhibiting muscle production and maintenance. Peptibodies, as a class of therapeutics, are well-characterized, with one product on the market and several more, including PINTA 745, in clinical trials. Compelling features of the PINTA 745 peptibody are its:
| • | demonstrated ability to promote muscle growth; |
| • | anti-inflammatory properties, a factor that we believe will be important due to the critical role that inflammation plays in PEW and the overall declining health of ESRD patients; and |
| • | dosing schedule, which conveniently aligns with dialysis treatment schedules. |
We believe that the mechanism and pharmacologic properties of PINTA 745 are well suited to the PEW setting. Preclinical and clinical data describing the effects of PINTA 745 are discussed below.
67
Preclinical Studies
A preclinical study was conducted to determine PINTA 745’s effect in mouse models of ESRD. In the 5/6th-nephrectomy model, a mouse model considered to be the industry standard for studying ESRD and its related effects, PINTA 745/s was shown to reverse body weight loss and reduce skeletal muscle mass and inflammation, which are morbidities associated with PEW. Nephrectomized mice, which have a condition mimicking ESRD and are referred to as CKD mice, and control mice of comparable size and blood urea nitrogen levels were injected either with PINTA 745/s or with saline. The experimental mice were injected subcutaneously at 5.0 mg/kg every other day for 7 to 28 days.
After seven days of PINTA 745/s treatment, the body and muscle weights of the CKD mice increased significantly compared with those in saline-treated CKD mice, an effect that persisted over 28 days.
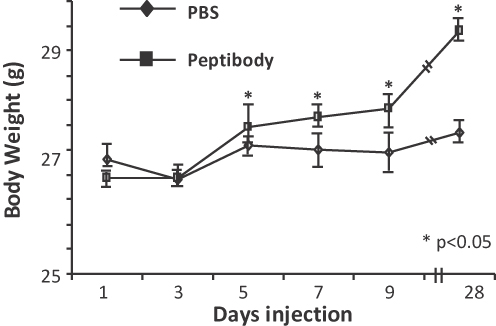
Protein synthesis—as measured by the uptake of a radiolabeled amino acid tracer—was increased and protein degradation—as measured by the release of a different amino acid tracer—was inhibited. This data underscores PINTA 745/s’ role in both forming new muscle and hindering the destruction of existing muscle.
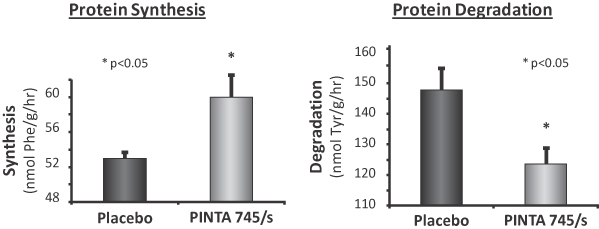
68
Further, PINTA 745/s increased muscle mass in the two muscles tested after seven days of treatment, the tibialis anterior and the gastrocnemius, an effect that continued over 28 days. In other preclinical studies, increases in muscle mass were observed in mice in doses as low as 0.01 mg/kg, with peak effect at 1.0 and 5.0 mg/kg.
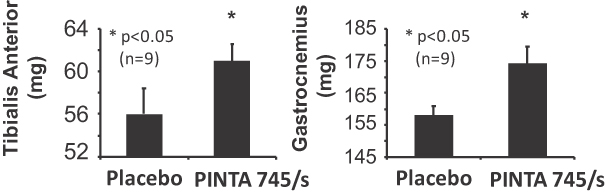
In CKD mice, circulating levels of 10 cytokines, which are mediators of inflammation, were increased in comparison to control mice. PINTA 745/s treatment for seven days decreased the level of these cytokines, suggesting that myostatin inhibition affects CKD-induced inflammation. The five cytokines shown below were the ones that were statistically significantly reduced in CKD mice treated with PINTA 745/s as compared to CKD mice treated with placebo.
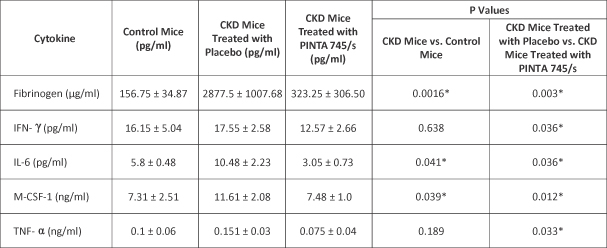
* Statistically significant.
Based on these observations, we believe that PINTA 745 has the potential to mitigate the effects of PEW in ESRD patients by increasing muscle formation, stimulating the conversion of muscle stem cells into muscle cells, and decreasing muscle destruction.
Furthermore, we believe that PINTA 745 has the potential to decrease inflammation in ESRD patients with PEW, which is an important potential factor often observed with greater morbidity and mortality.
PINTA 745 Phase 1 Clinical Studies — Safety and Tolerability
To date, three Phase 1 studies of PINTA 745 have been conducted, two in healthy volunteers and one in prostate cancer patients. We believe PINTA 745 showed an adequate safety and tolerability
69
profile in all three Phase 1 studies. Across all studies, which enrolled a total of 151 subjects, 48 subjects were exposed to the highest subcutaneous dose of 3.0 mg/kg and no treatment-related serious adverse events were observed. In the healthy volunteer trials, there were observations of some adverse events, mild in severity, that were not dissimilar to those observed in the placebo control group. No serious adverse events, discontinuations due to adverse events or deaths were reported in these trials. The only identified risk from the trials was injection site reactions, which can occur with agents dosed subcutaneously. In the Phase 1 study in prostate cancer patients, events were also mild in severity and similar in the PINTA 745 and placebo groups; one serious adverse event was reported that was considered not related to the drug. As a result, we believe PINTA 745 showed acceptable levels of safety and tolerability.
PINTA 745 Phase 1 Study in Prostate Cancer Patients
A multidose, placebo-controlled, double-blind Phase 1 study of PINTA 745 was carried out by Amgen on 54 men with prostate cancer who were receiving androgen deprivation therapy. This trial assessed both safety and efficacy following four weekly subcutaneous injections. Three Phase 1 dose groups were studied at dose levels of 0.3 mg/kg, 1.0 mg/kg and 3.0 mg/kg, with one placebo arm. This study was published in 2014 in The Journal of Clinical Endocrinology and Metabolism.
Efficacy parameters that were measured in this study included lean body mass as measured by dual energy X-ray absorptiometry, or DEXA, and lower-extremity muscle size as measured by CT scan. These methods are considered industry standard imaging techniques for measuring muscle mass or volume. Formal statistical testing for efficacy was conducted in the 3.0 mg/kg group. These statistical tests were not performed in the 0.3 mg/kg group and the 1.0 mg/kg groups because fewer patients were treated at these dose levels than were required for such analyses.
Lean body mass increased significantly in the 3.0 mg/kg dose group. The difference in lean body mass in the PINTA 745 group compared to the placebo group was approximately 2% greater at the end of the treatment period, a difference that increased over the subsequent four weeks of observation after the cessation of treatment, as shown in the following chart. Measurements for both placebo and PINTA 745 were taken at end of study, or EOS, at day 29, and at follow-up, or FUP, one month after day 29. There was a statistically significant increase in lean body mass at both EOS and FUP for the active arm compared to the control arm. Notably, lean body mass increase persisted at FUP, even without administration of the drug during the follow-up period.
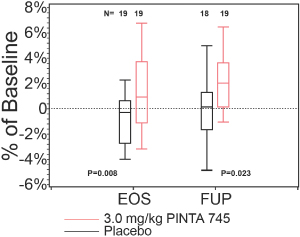
The bottom and top of the boxes represent the first and third quartiles, and the horizontal band inside the box indicates the median value. The ends of the whiskers indicate the minimum and maximum data in the range of observations.
70
As measured by CT scan, lower extremity muscle size increased significantly in the 3.0 mg/kg group. The muscle size increased in this group by approximately 1.2% at EOS, and further increased to 2.7% from baseline at FUP.
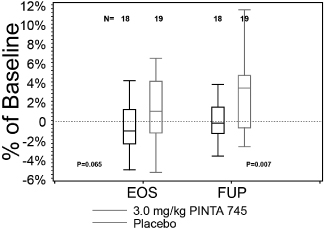
The bottom and top of the boxes represent the first and third quartiles, and the horizontal band inside the box indicates the median value. The ends of the whiskers indicate the minimum and maximum data in the range of observations.
Body fat decreased by 1.7% (p=0.021) in the 3.0 mg/kg group at the end of the treatment period compared to baseline, and the decrease was similar (1.5%, p=0.183) four weeks after the cessation of treatment. The decrease in body fat may reflect the presence of myostatin receptors in fat tissue. Reduced fat mass is an expected pharmacologic finding of myostatin inhibition, observed in multiple preclinical studies using PINTA 745/s as well as in three studies reported in the literature in which ActR2B-Fc fusions were used to inhibit myostatin. All of these studies, published in the International Journal of Obesity in 2009, the journal Endocrinology in 2012 and the journal Diabetologia in 2012, observed reduced fat accumulation in high fat fed mice.
In exploratory efficacy analyses comparing treatment effect and exposure across the dose groups, the 3.0 mg/kg dose appeared to have more impact on lean body mass than the lower doses, which suggests that humans exhibit dose-responsive efficacy from treatment with PINTA 745. This will be investigated in our ongoing clinical trial.
This trial was carried out in a rigorous setting in order to highlight the properties of PINTA 745. We believe that the results were clinically meaningful for the following reasons:
| • | The increase in muscle mass was statistically significant against the placebo group, with gains of 2% or more observed in response to treatment with PINTA 745. |
| • | The increase in muscle mass was seen after only one month of weekly dosing and persisted beyond treatment (one month following EOS). |
| • | The patients participating in this study were suffering from prostate cancer, which is associated with significant muscle loss. Historical control patients lost as much as 4% of muscle mass over a 12-month period, based on a study published in the journal Urology in 2004. |
Design of Ongoing Phase 2 clinical trial of PINTA 745 in ESRD patients with PEW
Our ongoing, randomized, double-blind, placebo-controlled trial with PINTA 745 is designed to demonstrate the effect of myostatin inhibition in PEW and lay the foundation for future clinical development. The study will enroll 48 patients, who will be randomized three-to-one (PINTA 745-to-
71
control). PINTA 745 will be given for three months, and then patients will participate in a two-month observation period to assess the durability of changes in muscle and inflammation. The primary endpoint of the trial is change in muscle mass seen through radiographic studies at three months versus the control group.
In the current Phase 2 trial in dialysis patients, we are seeking to reproduce and further characterize the muscle-building effect that was observed in prostate cancer patients in the Phase 1 study. To this end, we have made several key changes to the protocol to gain more insight regarding the efficacy and durability of responses.
| Design Element | Prior Phase 1 (Prostate) | Current Phase 2 (PEW) | Rationale | |||
| Route of Administration | Subcutaneous Injection | Intravenous Injection | Enhances drug exposure and aligns with routine patient management in the dialysis setting | |||
| Duration of Therapy | 1 month | 3 months | Longer-term dosing may enhance muscle growth | |||
| Dose of PINTA 745 | 0.3, 1 and 3 mg/kg given weekly | 3 mg/kg weekly; 3 mg/kg loading dose followed by 1 mg/kg maintenance dose; and 6 mg/kg loading dose followed by 2 mg/kg maintenance dose | Higher drug exposure may be more effective while similarly well tolerated | |||
| Duration of follow up | 1 month | 2 months | Extends information on durability of effect | |||
We also have included two functional muscle assessments as secondary endpoints that were not included in the Phase 1 studies.
We will be using stair climbing power and six-minute walk tests in order to identify the appropriate parameters to use for physical function testing in future trials. These assessments have become significantly more common in clinical trials and have formed the basis for regulatory approvals of other agents in different indications. Because these assessments were developed for other patient groups of similar age and functional muscle status, such as patients recovering from a heart attack, we believe that these endpoints are appropriate for use in this population. Once we have demonstrated their feasibility, we may choose one or both of these physical functional assessments for endpoint data in later-stage clinical trials.
Other assessments in the trial include:
| • | Demonstration of the feasibility of quality of life assessments, such as the kidney disease quality of life assessment as well as assessments of fatigue and anorexia/cachexia. |
| • | Safety monitoring and exposure, including pharmacokinetics, or PK. |
| • | Effects on the duration of use and dose intensity of supportive care drugs. |
72
Given the robust design features of the Phase 2 trial protocol, we believe that if this trial is successful, it will confirm the potential clinical utility of PINTA 745 in this patient population and help us appropriately design subsequent clinical trials to support applications for regulatory approval.
The design of our Phase 2 trial was created not only to support eventual regulatory approval but also to be able to pilot the assessments that will be needed to obtain reimbursement. For that reason, we chose trial sites that effectively reflect the etiology of ESRD in the United States. Our six sites include academic sites, as well as those associated with DaVita and Fresenius. These centers are representative of the vast majority of the US dialysis market.
Biomarker Approach
As part of our Phase 2 clinical trial protocol, we are measuring serum levels of myostatin in patients to see if we can use it as a biomarker to predict which patients will respond best to treatment.
Status of Ongoing Phase 2 clinical trial of PINTA 745 in ESRD patients with PEW
As pre-specified by the protocol, we conducted a review of all available safety data when the first eight patients at the 3 mg/kg weekly dose level had completed one month of treatment. At that time, we observed no dose-limiting toxicities, no treatment-related serious adverse events nor grade 3 or higher adverse events and no anti-drug antibody formation. Adverse events that were deemed possibly related to treatment with PINTA 745 at that time were all grade 1 or 2 in severity, with muscle pain as the most commonly reported treatment-related adverse event. The safety committee, consisting of the clinical trial sponsor and the trial investigators, considered the 3 mg/kg weekly dose to be safe and well tolerated and determined that it would be appropriate to proceed with protocol-specified cohort expansion and dose escalation. In addition, pharmacokinetic data from these first eight patients showed that PINTA 745 has a longer half-life in ESRD patients compared with previously studied healthy volunteers and men with prostate cancer. Drug exposure levels in PEW patients at 3 mg/kg were similar to those predicted for 10 mg/kg based on the prior Phase 1 experience. This pharmacokinetic data also showed that an administration schedule consisting of loading doses followed by maintenance doses is appropriate for this patient population in order to rapidly achieve steady-state levels of PINTA 745. As a result, we amended the protocol to incorporate new dosing regimens to:
| • | enroll a cohort of 20 patients who are receiving a loading dose of 3 mg/kg given weekly for three weeks, followed by treatment for an additional nine weeks with a dose of 1 mg/kg given weekly, a regimen that is anticipated to provide drug exposures in PEW patients similar to those achieved in prostate cancer patients who showed statistically significant improvements in lean muscle mass; and |
| • | enroll a cohort of 20 patients who are receiving a loading dose of 6 mg/kg given weekly for three weeks, followed by treatment for an additional nine weeks with a dose of 2 mg/kg given weekly, to escalate exposure and explore efficacy and safety at a higher dose level. |
Likewise, as pre-specified by the protocol, we conducted a review of all available safety data when the first eight patients at the 6 mg/kg weekly loading dose followed by 2 mg/kg weekly maintenance dose level had completed one month of treatment. To date, we have observed no dose-limiting toxicities, no treatment-related serious adverse events nor treatment related grade 3 or higher adverse events, no anti-drug antibody formation, and no unexpected laboratory findings. Adverse events that were deemed possibly related to treatment with PINTA 745 were all grade 1 or 2 in severity, with muscle pain as the most commonly reported treatment-related adverse event. The safety committee, consisting of the clinical trial sponsor and the trial investigators, considered the 6 mg/kg weekly loading dose followed by 2 mg/kg weekly maintenance dose to be safe and well tolerated and
73
determined that it would be appropriate to proceed with protocol-specified dose expansion. Additionally, available pharmacokinetic data supported the transition to the loading dose/maintenance dose regimens in that steady state concentrations of PINTA 745 were rapidly achieved and drug accumulation was not observed.
Additional Opportunities for PINTA 745
We designed the Phase 2 trial to give us insight into potential additional markets for PINTA 745. Those markets could include: orthopedic indications; inflammation and inflammatory disease; age-related sarcopenia; and cancer cachexia. In each of these conditions, we believe muscle growth and reduction in inflammation resulting from treatment with PINTA 745 could lead to better outcomes. As additional data from our clinical and preclinical studies with PINTA 745 emerge, we may initiate clinical studies in other indications. For example, given that preclinical studies suggest that myostatin inhibition has the potential to improve the metabolism of glucose in the body, we plan to initiate a pilot clinical study to assess the effects of PINTA 745 on glucose and fat metabolism.
STM 434, a Targeted Therapy for Ovarian Cancer and Potentially Other Solid Tumors
STM 434 is in a Phase 1 clinical study in ovarian cancer and other solid tumors, which commenced in 2014. STM 434 is a soluble ActR2B receptor-IgG fusion protein that binds the signaling molecule human activin. STM 434 has the potential to be the first product to target tumor growth and proliferation by inhibiting multiple ActR2B ligands, including Activin A. A ligand is a protein that binds a receptor on a cell to trigger a signal. In ovarian cancer, Activin A is a novel and promising target. Published data, including a study in Clinical Cancer Research in 2008, as well as our preclinical data, suggest that Activin A is upregulated in patients with ovarian cancer, and blocking it reduces proliferation of tumor cells. In many solid tumor types, upregulation of Activin A is correlated with poorer prognoses.
Ovarian Cancer
Ovarian cancer is the fifth leading cause of cancer death in women in the United States. According to the National Cancer Institute, there were an estimated 22,240 new ovarian cancer cases and 14,030 ovarian cancer deaths in the United States in 2013. Surgery and cytotoxic chemotherapies are widely used to treat ovarian cancer; however, the outcomes have changed little in 40 years. There were estimated to be approximately 186,000 women suffering from ovarian cancer in the United States in 2010. According to the American Cancer Society, based on patients diagnosed between 2003 and 2009, the blended five-year survival rate is only 44% for ovarian cancer patients overall.
Ovarian cancers are divided into three distinct main subtypes:
| • | serous adenocarcinoma, which accounts for approximately 63% of ovarian tumors in the United States; |
| • | clear cell cancers, which account for approximately 11% of ovarian tumors in Western countries and a higher percentage in Asian countries. For example, clear cell cancers have been reported to account for approximately 23% of ovarian tumors in Japan; and |
| • | granulosa cell tumors, which account for approximately 2 to 5% of ovarian tumors in the United States. |
74
Limitations of Current Therapies for Ovarian Cancer
Despite the strong unmet need for better therapies, there have been few new treatment options introduced, and numerous studies, including a 2012 study published in Obstetrics & Gynecology, have shown that clinical outcomes have not improved significantly for several decades.
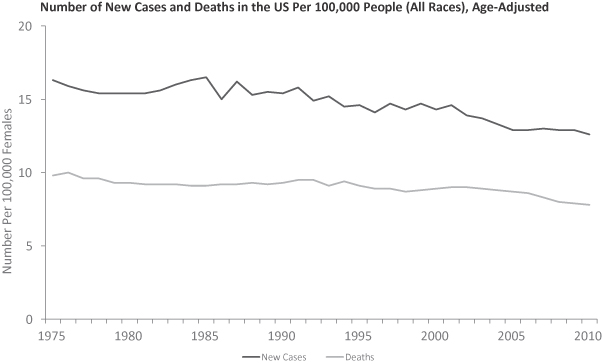
First Line Treatment
Surgical therapy for ovarian cancer that has not escaped the ovary can be curative. In other cases, palliative debulking surgery is often considered. However, for women with advanced or recurrent tumors that have escaped the ovary and involve critical anatomic structures, there are no curative therapies, and chemotherapy is generally employed. When chemotherapy is indicated, treatment for these subtypes may vary but are generally based on a foundation of platinum chemotherapy. Response rates and outcomes vary among subtypes.
| • | Serous tumors have a reported response rate to chemotherapy of 72 to 73%, according to a 2005 study in the journal Clinical Cancer Research; however, most patients relapse, resulting in a median survival of approximately 40.8 months, according to a 2010 publication in the International Journal of Gynecological Cancer. |
| • | Clear cell tumors have a platinum-based chemotherapy response rate of approximately 11% as reported in a 2006 study in the British Journal of Cancer. Median overall survival in patients with clear cell tumors is approximately 21.3 months. |
| • | The data on post-surgery response rates to chemotherapy in the granulosa subtype of ovarian cancer is limited due to its rarity. |
Recurrent Disease Treatment
For patients whose tumors did not respond to first line therapy, or for those whose tumors became unresponsive to platinum chemotherapy, a number of other chemotherapy options may be
75
applied, including liposomal doxorubicin, topotecan and gemcitabine. Despite these therapies, the median survival of platinum chemotherapy resistant ovarian cancer is approximately 13 months.
Role of Activin A in Ovarian Cancer and Other Solid Tumors
Activin A, a secreted growth factor, is a member of the TGF-ß superfamily of growth factors, which also includes Activin B, Activin AB, GDF-11 and others. Activin A is widely understood to be involved in the growth and proliferation of ovarian cancer and other solid tumors. Some of the other secreted proteins in this superfamily, including Activin AB, have also been implicated in the growth of these tumors. As reported in BMC Medical Genomics in 2010, overexpression of Activin A in support cells called stroma is a key component of a metastasis-associated gene expression signature. This signature predicts shortened survival across a number of cancers including, among others, ovarian, gastric and breast cancers. Overexpression of Activin A is now recognized as a common feature across advanced solid tumors including head and neck, colon, gastric, esophageal, pancreatic and non-small cell lung cancer. In addition to their role in regulating interactions between epithelial cells and stromal cells, activins may also be involved in regulating stem cell survival.
Activin A has been found to play a role in the three principal subtypes of ovarian cancer: serous, clear cell and granulosa. For example, the mRNA precursor for activin has been found to be upregulated in approximately 30% of specimens of serous ovarian cancer. At the protein level, as published in 1997 in the Journal of Clinical Endocrinology and Metabolism, most typical serous ovarian cancers made serum Activin A.
Many women with ovarian cancer have high levels of Activin A. The utility of high Activin A in ovarian cancer will be explored in the Phase 1 study.
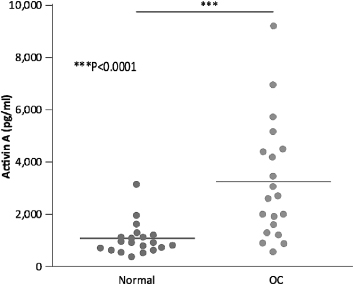
Genetic Linkages to Ovarian Cancer Subtypes
In a genetic link between the activin pathway and ovarian cancer, mutations in the BRCA gene have been found in 5 to 10% of serous ovarian tumors. According to a 2012 publication in the journal PloS One, these patients with BRCA mutations fail to produce the Activin A counter-regulators follistatin and inhibin, implying that these tumors may be unable to switch off activin signaling.
In clear cell ovarian cancer, studies have shown that mutations in the ARID1A gene contribute to tumor proliferation.
76
Specifically, these mutations drive upregulation in the signaling cascade triggered by the ActR2B receptor. Mutations in the ARID1A gene were present in 55 of 119 (46%) and 17 of 31 (55%) ovarian clear cell tumors, as reported in a 2010 publication in The New England Journal of Medicine and a 2014 publication in BMC Cancer, respectively. We believe that increased levels of activin mimic the effect of ARID1A mutations, and therefore play a similar role in clear cell ovarian cancer.
In granulosa cell ovarian cancer, mutations in the FOXL2 C134W gene have been suggested in several studies to drive the growth of tumors. This mutation was present in 97% (86 of 89) of granulosa cell tumors as reported in a 2009 publication in The New England Journal of Medicine. In a normal cell, activin is under tight control—FOXL2 protein turns on follistatin when an activin signal is received, and follistatin, a natural inhibitor of activin, then shuts off the activin signal. However, in granulosa cell tumors, mutant FOXL2 C134W is not able to turn on follistatin, and activin signals continue unchecked. These studies have been reported in 2014 in the journal Biochemical and Biophysical Research Communications as well as in 2013 in the journal Molecular and Cellular Endocrinology.
Mechanism of Action of STM 434
We believe that STM 434 has the potential to be the first product to address directly the underlying biology of ovarian tumors.
Activin A is known to act through the ActR2B receptor on the surface of ovary cells. When the receptor receives the signal from Activin A, it initiates a cascade of gene transcription that leads to abnormal cell proliferation, cell migration, blood vessel formation and inhibition of programmed cell death. STM 434 is a ligand trap, which mimics the ActR2B receptor, binding Activin A and other ligands that would normally activate this receptor. Several ligand traps based on other receptors have been developed as therapeutic products and commercialized successfully. The choice of a ligand trap for STM 434 conforms mechanistically with the goal of binding Activin A and other secreted proteins associated with the ActR2B receptor and tumor growth.
STM 434 has a half-life of one to two weeks in monkeys. We initiated dosing of STM 434 every four weeks in our ongoing Phase 1 study. This dosing schedule would align well with the current predominant protocols for administering chemotherapy in both the first-line and the second-line setting in ovarian cancer, which range from weekly to monthly.
Preclinical Studies
Preclinical testing of STM 434 was designed to confirm and quantify its effects in binding Activin A and other ligands with a receptor-like ligand trap. These studies were conducted with STM 217, a close analog of STM 434, which we refer to as STM 434/s. In addition, these studies were carried out in two types of mouse models: TOV-21G mice, which are analogous to patients with clear cell ovarian tumors and carry ARID1A mutations, and inhibin knockout mice, which are analogous to patients with granulosa cell tumors.
Results of the TOV-21G study have shown that blocking Activin A by using a soluble receptor, as both a single therapy and in combination with chemotherapy, led to a reduction in tumor size. In other experiments, knockout mice that were born without inhibin, and therefore had high activin levels that led to granulosa cell ovarian tumors, survived longer after treatment with STM 434/s in comparison to untreated mice. A 2007 publication in the journal Molecular Human Reproduction showed that the survival of the knockout mice was greatly improved when they were treated with an ActR2B-Fc fusion similar to STM 434. Other mouse tumor models tested, including renal cell carcinoma, melanoma and small cell lung cancer were shown to be sensitive to activin levels and antitumor responses were seen when activins were inhibited.
77
TOV-21G Mouse Models (Clear Cell Ovarian Tumors)
In a preclinical study using TOV-21G mice, tumors derived from human clear cell ovarian carcinoma were shown to have high levels of serum Activin A, analogous to those observed in human ovarian cancer patients as described above.
Serum Activin A
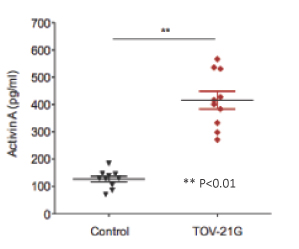
In a subsequent preclinical study that we presented together with Amgen at the American Society of Clinical Oncology meeting in Chicago in 2013, we evaluated STM 434/s in this TOV-21G model used as both a single agent and in combination with the chemotherapy agent 5-fluorouracil, or 5-FU. STM 434/s was administered subcutaneously weekly at 10.0 mg/kg beginning on day 12. 5-FU was administered for three cycles. The tumor was measured two to three times per week, up to day 52. Results from these experiments showed a statistically significant (31%, p<0.0001) reduction in tumor volume for the agent. Results of the combination experiments showed an additive (73%, p<0.0001) reduction in tumor growth.
Additive Effect with 5-FU
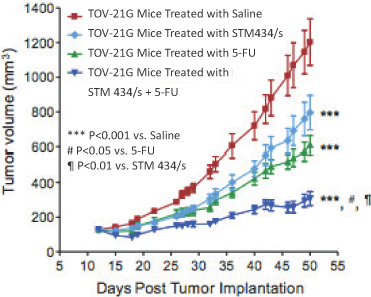
78
In addition, this study examined the anticachectic effects of STM 434/s in this model. Cachexia is a condition associated with significant weight loss often seen in patients with solid tumor cancers. The results of this study showed that the administration of STM 434/s increased body weight of the mice. In addition to demonstrating the antitumor properties of STM 434/s, we believe that this data also demonstrates that an ActR2B soluble receptor may provide an additional benefit to patients by addressing cancer cachexia. We intend to investigate these attributes as part of our planned Phase 1 clinical study.
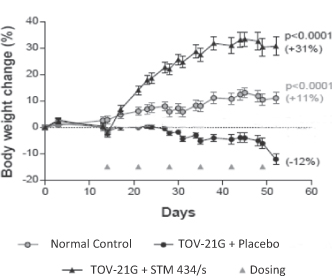
Inhibin Knockout Mouse Model (Granulosa Cell Tumors)
For granulosa cell studies, a knockout mouse model was used with STM 434/s. The study showed that serum Activin A levels in the knockout mice were elevated, and upon treatment with STM 434/s Activin A levels were significantly reduced.
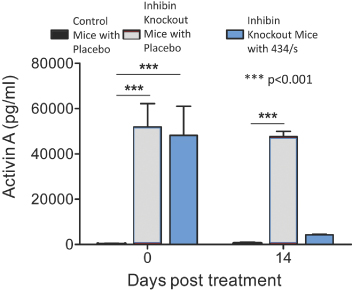
STM 434/s treatment reduced the elevated circulating Activin A in the inhibin knockout mice to the levels in control mice. Serum Activin A was measured before and 14 days after treatment.
79
Further, this study showed that treatment with STM 434/s reduced ovary size to near normal in comparison to control mice treated with saline. A representative example of the observed reduction in size is shown below. In this study, STM 434/s was administered as a single dose of 30 mg/kg.
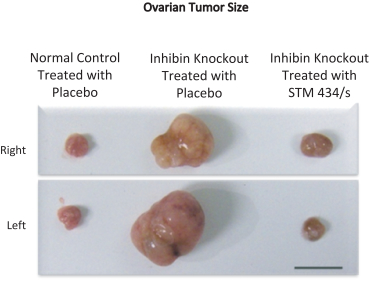
Lastly, the knockout model treated with STM 434/s showed a statistically significant (p<0.0001) improvement in survival with 90% (20 of 22 mice) alive at 133 days of age, as compared to knockout mice treated with saline, where 96% (23 of 24) had died by this time.
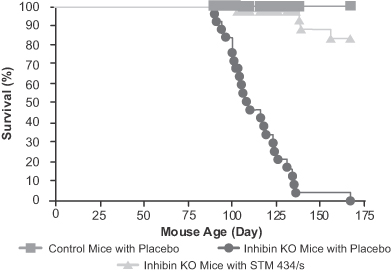
In July 2014, Amgen provided us a draft report from a 2009 eight-week pharmacology study of STM 217, a compound closely related to STM 434 and which we also refer to as STM 434/s, in orchiectomized (neutered) male cynomolgus monkeys. This pharmacology study was designed to explore the ability of STM 217 to reverse the effects of androgen deprivation. In the study, two weekly doses of STM 217 were evaluated at 3 mg/kg and 10 mg/kg. The study found that STM 217 was effective in mitigating the muscle and bone loss that accompany androgen deprivation in this animal model.
80
In addition to the muscle and bone effects, clinical observations from the study included bleeding from the muzzle (similar to human nosebleeds) in some of the monkeys and one animal bleeding from a skin lesion over the buttock. In this study, it was not possible to determine if the bleeding was caused by STM 217. To further characterize this observation, we performed additional in vitro studies of STM 217 and STM 434. Platelets, a component of blood that helps stop bleeding, were evaluated, and neither STM 217 nor STM 434 impacted platelet function. We also evaluated BMP-9, a factor involved in bleeding and blood vessel development known to be mutated in humans with hereditary hemorrhagic telangiectasia, or HHT. Both STM 217 and STM 434 bound to BMP-9 in these studies, suggesting that the bleeding observed with STM 217 could also be observed with STM 434. The observations from the STM 217 report and the in vitro studies we conducted have been shared with the FDA.
As a result of these findings with STM 217, we altered our STM 434 Phase 1 study protocol to exclude patients at heightened risk of bleeding and enhance the monitoring of patients for bleeding or increased risk for bleeding. These changes were also shared with the FDA.
Phase 1 Clinical Study in Ovarian Cancer and Other Solid Tumors
We commenced an open-label Phase 1 study of STM 434 in 2014 that will enroll approximately 66 patients, assuming all cohorts are expanded to the maximum number of patients allowed. The initial dosing schedule for this study is once every four weeks. This study is being conducted in three parts:
| • | Part 1 — Dose escalation study in patients with advanced solid tumors. Dosing initiated at 0.25 mg/kg. We plan to test up to the maximum tolerated dose, or MTD. Assuming no MTD is reached, we will test ascending doses of STM 434. |
| • | Part 2 — Designed to obtain additional safety and exploratory efficacy data in patients with advanced ovarian cancer, including clear and granulosa cell tumors. |
| • | Part 3 — Designed to study STM 434 in combination with chemotherapy in patients with ovarian cancer who have received prior treatment. |
The objectives for our Phase 1 study are: to test if STM 434 monotherapy is safe and well tolerated; to obtain preliminary efficacy data in ovarian cancer and other solid tumors; to assess safety and preliminary efficacy of STM 434 with liposomal doxorubicin chemotherapy or the current standard of care; and to explore biomarkers predictive of response to treatment. Further objectives include collecting pharmacokinetic data during therapy with STM 434 and defining the recommended Phase 2 dose.
Since initiating this study in October 2014, we have continued to dose and enroll patients. Bleeding has been observed in a subset of patients. Some of these bleeding events were deemed by the treating investigators to be possibly related to treatment with STM 434. Following review of these events by the safety committee, consisting of the trial sponsor and the trial investigators, the associated doses were deemed safe and well tolerated, and the study is continuing at escalating doses.
Based on data supporting the role of activin in the progression of other solid tumors and the inclusion criteria, we expect that two-thirds of the patients included in the dose escalation portion of the Phase 1 study will have solid tumors in organs other than the ovary. A portion of the other tumors may include pancreas, stomach and kidney tumors, where there is a high correlation between Activin A upregulation and the severity and outcome of disease. We expect to release initial data from this Phase 1 clinical study in the first half of 2016.
81
Biomarker Approach
Activin expression is one of a few biomarkers associated with severity in a variety of tumors including ovarian tumors. For this reason, Activin A is one of 12 genes that are measured in colon cancer as part of the clinically validated OncotypeDX colon cancer panel. Our Phase 1 study is testing whether high levels of Activin A measured at baseline before patients receive STM 434 predict whether they respond to treatment. If levels of Activin A can predict response, this biomarker may be valuable in late-phase trials to improve the trial design and maximize the proportion of patients who respond to STM 434.
In addition, we will be measuring follicle-stimulating hormone, or FSH, levels, a routine laboratory test, to determine the inhibition of activin by STM 434. It is well established that activin negatively regulates FSH, and we therefore can use FSH reduction as a surrogate for activin inhibition. We also plan to conduct ARID1A and FOXL2 mutation testing in our Phase 1 study. These mutations have been associated with tumor proliferation.
Molecularly Targeted Product Candidate Pipeline
Our molecularly targeted product candidate pipeline currently consists of five product candidates that were licensed from Amgen in addition to PINTA 745 and STM 434. The members of this initial portfolio are closely related to one another in terms of the biology and align with our in-house expertise regarding development, manufacturing, intellectual property strategy and other critical activities. These products share association with the TGF-ß superfamily of growth factors. At the same time, they represent distinct modes of intervention with potentially different therapeutic applications. These distinctions relate to target specificity, pharmacokinetic/pharmacodynamic relationships and modality. We believe these product candidates have unique characteristics, and, in some cases, demonstrated activity in preclinical studies, which would make them attractive candidates for various indications, including cancer cachexia, a condition that is implicated in up to 30% of cancer deaths with limited existing treatments. We are evaluating these product candidates to determine the best path forward. Where appropriate, we intend to conduct preclinical studies and file IND applications with regulatory authorities for these candidates. For example, we are conducting IND-enabling manufacturing and preclinical studies for ATA 842.
Our molecularly targeted product candidate pipeline licensed from Amgen includes the following:
| • | ATA 842, a humanized antibody targeting myostatin designed to be more selective than similar programs in the clinic targeting oncologic, orthopedic and renal indications; |
| • | ATA 777, a fully human antibody targeting Activin A, which we believe will be well suited for non-oncology indications where chronic dosing and specificity to Activin A is beneficial; |
| • | ATA M43, a fully human anti-ActR2A/2B monoclonal antibody with high affinity to both receptors that is mechanistically similar to programs targeting muscle wasting diseases; |
| • | STM 217, a soluble ActR2B receptor-IgG Fc fusion protein and a close analog of STM 434; and |
| • | ActR2B5, a soluble ActR2B receptor that can be fused to an IgG Fc receptor. |
Our T-Cell Product Candidates
T-cells are a critical component of the body’s immune system and can be harnessed to counteract viral infections and some cancers. By focusing the T-cells on specific proteins involved in cancers and infections, the power of the immune system can be employed to combat these diseases. In June 2015, we exclusively licensed from MSK worldwide rights to three clinical stage T-cell product candidates. We also have an exclusive option to exclusively license from MSK worldwide rights to certain other T-cell programs that are discovered or developed by MSK pursuant to sponsored research funded by us.
82
Our T-cell product candidates arise from a platform technology designed to produce off-the-shelf, cellular therapeutic options for patients with unmet medical needs. Our initial T-cell product candidates target viral- or cancer-specific antigens.
Our most advanced T-cell product candidate, EBV-CTL, is in Phase 2 clinical trials for the treatment of EBV-associated malignancies. EBV is the virus that causes mononucleosis and is associated with a number of more severe diseases, including certain malignancies and neurologic conditions, such as multiple sclerosis, or MS. EBV-CTL received Breakthrough Therapy designation from the FDA in February 2015 for the treatment of patients with rituximab-refractory EBV-LPD after HCT, based on data from two separate clinical trials conducted by MSK. Since licensing our T-cell product candidates, the IND under which these studies were conducted has been transferred to us. We recently met with the FDA to discuss late-stage development to support a potential approval in this indication. Based on guidance from the FDA, we intend to conduct a pivotal study in rituximab-refractory EBV-LPD after HCT and expect to submit a special protocol assessment for this pivotal study. In addition, we had preliminary discussions with the FDA regarding late-stage development in the setting of rituximab-refractory EBV-LPD after SOT, and we will be incorporating this feedback into our subsequent development plans in this indication.
Our second T-cell product candidate, CMV-CTL, targets CMV, an infection that can result in blindness, illness or death, depending on the tissue it affects, in those with weakened immune systems. CMV is also associated with certain malignancies, including glioblastoma multiforme, or GBM. CMV-CTL is currently being investigated in Phase 2 clinical trials sponsored and conducted by MSK for CMV infections that occur in some patients who have received an HCT.
Our third clinical stage T-cell product candidate, WT1-CTL, targets WT1. Abnormal expression of WT1 is seen in a variety of hematologic and solid tumors, including multiple myeloma, acute myeloid leukemia, and ovarian cancer. This product candidate is currently in Phase 1 clinical trials sponsored and conducted by MSK.
83
Clinical experience with our T-cell product candidates is broad, including in immunocompromised states, as well as in solid and hematologic malignancies. Selected data from clinical studies of our three T-cell product candidates are summarized in the table below.
| T-Cell Program |
Stage | Indication | Recent Clinical Data Highlights |
Number of Patients Who Received Prior Therapy |
Historical Outcomes Data | |||||
| EBV- CTL |
Phase 2 clinical trials | EBV lymphoma (EBV-LPD) following allogeneic hematopoietic cell transplantation (HCT) from bone marrow or cord blood | 62% response rate in 26 patients treated with EBV-CTL derived from primary HCT donors with 16 complete responses (CR) and zero partial responses (PR) | 13 of 26 received prior rituximab | Historical median survival in rituximab refractory patients is 16-56 days | |||||
| 65% response rate in 34 patients treated with EBV-CTL derived from third-party donor, with 19 CRs and three PRs; one-year overall survival (OS) range 56.3-71.8% two-year OS range 46.9-63.8% |
All received prior rituximab | |||||||||
| EBV-LPD following solid organ transplantation (SOT) | 62% response rate in 13 patients treated with third-party derived EBV-CTL, with one CR, seven PRs two-year OS of 57.7% |
All received prior rituximab; 11 of 13 had received prior chemotherapy; 12 of 13 patients had high risk disease | Historical data show 33% OS at two years in patients with incomplete response to rituximab | |||||||
| CMV- CTL |
Phase 2 clinical trials | Post-HCT anti-viral drug resistant CMV viremia (high viral count) and symptomatic CMV disease | 64% response rate in 25 CMV viremia patients treated with third party derived CMV-CTL, with nine CRs and seven PRs; 67% response rate in nine CMV disease patients, with five CRs and one PR |
All received prior antiviral therapy; median of four prior therapies including experimental therapies | Uncontrolled CMV disease leads to high rates of morbidity and mortality (for example, CMV pneumonitis confers a four fold higher risk of death) | |||||
| WT1- CTL |
Phase 1 clinical studies | Various cancers, including acute myeloid leukemia (AML), multiple myeloma | Data not yet available | Not Applicable | Not Applicable | |||||
84
Efficacy and safety data for both EBV-CTL and CMV-CTL have been published in the journal Blood and presented at major scientific conferences. We are focusing our initial development and regulatory activities on EBV-CTL in the post-HCT and post SOT-setting and CMV-CTL in the post-HCT setting, which we believe offer a rapid path to marketing approvals if supported by additional clinical data. However, we intend to concurrently explore the clinical utility of our T-cell product candidates in other relevant disease states.
T-cell Technology Platform
Our T-cell product candidates share a common technology under which T-cells are collected from the blood of third-party donors and then exposed to a selected viral antigen in order to activate them against that particular virus. The resulting activated T-cells are expanded in number, characterized and stored for future therapeutic use in an appropriate partially human leukocyte antigen, or HLA, matched patient, providing an off-the-shelf, cellular therapeutic option for patients. Since these T-cells are off-the-shelf, patients often only need to wait days until they receive treatment. In addition to expanding the activated T-cells, the manufacturing process also leads to substantial reduction in the number of alloreactive cells, which cells can cause graft versus host disease, or GvHD. We believe this reduces the risk of GvHD, a serious complication in immunocompromised recipients.
The process through which EBV-specific T-cells, or EBV-CTLs, are generated is shown in the diagram below. First, B-cells derived from the blood of a third-party donor are exposed to a specific strain of the EBV virus to create EBV transformed B lymphoblastoid cell lines, or EBV BLCLs. The BLCLs are irradiated to prevent the BLCLs from growing and then co-cultured with T-cells derived from the blood of the same third-party donor. In this co-culture process, the BLCLs present EBV antigen to the T-cells to activate the T-cells against the EBV virus. These activated EBV-specific T-cells are then sensitized and expanded, while the potentially alloreactive cells contained in the same culture are not expanded. When complete, the cultures are assessed for EBV reactivity, HLA restriction, the absence of allo-specificity and microbial sterility. Once fully characterized in this way, the cell lines are cryopreserved and stored for future therapeutic use as an off-the-shelf therapy.
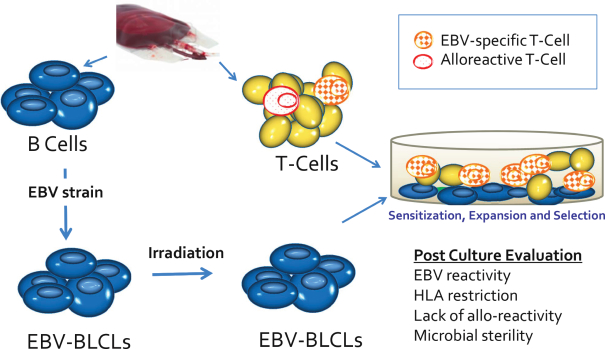
85
The donor’s blood contains a mix of T-cells, some that have the potential to target EBV-infected cancer cells and others, called alloreactive or allospecific T-cells, that have the potential to target cells recognized as foreign. Administration of bulk third-party lymphocytes that contain a relatively high proportion of allospecific T-cells has the potential to cause severe and life-threatening toxicities such as GvHD when these allospecific T-cells recognize the recipient’s native cells as foreign. Our manufacturing process enriches the product for the desired EBV-CTLs while depleting the undesirable allospecific T-cells as they are not stimulated to expand and eventually die. As shown in the table below, the existing manufacturing process typically results in an approximately 70-fold expansion in the number of EBV-specific T-cells and reduces by a factor of approximately 20 the number of GvHD-causing allospecific T-cells, compared with the prevalence of these two types of cells in a sample of bulk donor lymphocytes.
| Bulk Donor Lymphocytes | EBV CTL | |||||||
| EBV-Specific T-cells |
1,190 per million T-cells | 80,920 per million T-cells | ||||||
| Allospecific T-cells |
6,790 per million T-cells | 350 per million T-cells | ||||||
In addition to being evaluated for expansion before release for use in clinical studies, cells are also evaluated for HLA restriction. HLA restriction refers to the fact that any given T-cell line will only recognize such T-cell line’s target—in this case an EBV protein—when it is bound to a particular HLA. For example, an EBV-CTL restricted by a particular HLA known as HLA A*02:01 will only kill EBV-infected cells that show that same EBV protein when bound to HLA A*02:01. This process identifies EBV-CTLs that are specific to the desired target, limiting undesirable off-target killing of other cells.
An appropriate cell line for use in a particular patient is typically defined as being matched at two of eight HLA alleles and restricted through a shared HLA allele. In an analysis conducted by MSK and reported at the 2015 American Association for Cancer Research, or AACR, annual meeting, an appropriate cell line was determined to be available for all but one of 200 consecutive unrelated transplant recipients and 100 cord blood transplant recipients. This analysis was based on evaluating these potential patients against a bank of approximately 330 HLA characterized EBV-CTL lines that MSK has generated to date. MSK’s clinical experience has yielded an empirically derived, proprietary approach to selecting the appropriate cell line for use in individual patients. We believe this algorithm will ultimately allow us to deliver the therapy efficiently by focusing on a limited set of EBV-CTL lines without compromising our ability to treat a wide range of patients with diverse HLA types.
A similar process is used to generate and characterize CMV-CTL and WT1-CTL, and we also plan to utilize this process to generate diverse banks of targeted cytotoxic T-cell lines against other antigens of interest.
EBV Targeted T-Cells for EBV-LPD and Other EBV Associated Diseases
EBV is a member of the Herpes virus family and is one of the most common viruses in humans. It is present in all populations, infecting more than 95% of all individuals within the first four decades of life. In healthy individuals, EBV causes infectious mononucleosis, a generally benign self-limiting condition. Following the acute phase of EBV infection, the virus remains present in a small number of B-cells throughout the body; however, it is kept in check by the intact immune system. Though benign in the vast majority of people, EBV has been demonstrated to be involved in the development of many malignancies. In immunocompromised patients, EBV causes lymphomas and other lymphoproliferative disease collectively called EBV-LPD. EBV-LPD most commonly affects patients after HCT or after SOT. Even in patients with intact immune systems, EBV is associated with various hematologic malignancies and solid tumors including Hodgkin lymphoma, Burkitt’s lymphoma, other B-cell malignancies, nasopharyngeal carcinoma and gastric cancer. EBV is also associated with certain diseases of the central nervous system, including multiple sclerosis.
86
The estimated number of patients per year in the United States and European Union with EBV associated malignancies is highlighted in the figure below.
| Indication |
Estimated Number of Patients |
|||
| EBV-LPD after HCT |
1,300 | |||
| EBV-LPD after SOT |
1,700 | |||
| EBV positive Diffuse Large B cell lymphoma |
2,900 | |||
| EBV positive chemotherapy refractory Hodgkin Lymphoma |
2,100 | |||
| EBV positive nasopharyngeal carcinoma |
6,000 | |||
| EBV positive gastric cancer |
16,500 | |||
EBV-LPD after HCT
EBV-LPD is a rare but serious complication in recipients of HCT. EBV-LPD is often severe and sudden in onset and results in death in the majority of HCT patients who develop the disease. A study conducted by the Karolinska Institute that was reported in the journal Haematologica noted a three-year survival rate of just 20%. According to the 2012 report of the CIBMTR, there were 7,554 allogeneic transplants in the United States in 2012 and according to the European group for blood and marrow transplantation, there were 14,549 allogeneic transplants in the European Union. While autologous transplants, or those obtained from the same individual, still comprise the majority of all transplants in the United States and European Union, the relative proportion of allogeneic transplants, or those obtained from a third-party donor, has increased over time, and we believe this trend will continue due to the increasing utilization of haploidentical transplants and reduced intensity transplants.
The monoclonal antibody rituximab is typically used off-label to treat EBV-LPD, producing initial responses in approximately 55% of treated patients and durable responses in approximately 20% of treated patients. However, for those who relapse after rituximab therapy or fail to respond to rituximab, or for those with CD20 negative lymphoma (which is known to be unlikely to respond to rituximab), EBV-LPD is frequently lethal. For example, it was reported in 2014 in the journal Bone Marrow Transplantation that the median survival period from diagnosis of rituximab-refractory EBV-LPD in adult HCT patients was 33 days, and in 2014 it was reported in the journal Haematologica that median survival was 16 days. In 2008 it was reported in the journal Bone Marrow Transplantation that the median survival period from the time of diagnosis in a group of EBV-LPD patients who received rituximab was 56 days. Taken together, these studies suggest a range of median overall survival, or OS, in the setting of rituximab failure of 16-56 days.
MSK has conducted two separate clinical trials of EBV-CTL that enrolled a heterogeneous group of patients with a variety of EBV-associated malignancies, including, but not limited to, EBV-LPD after HCT and EBV-LPD after SOT: Study 95-024, initiated in 1995, and Study 11-130, initiated in 2011. Results from these two studies supported the granting of Breakthrough Therapy designation by the FDA for EBV-CTL in February 2015 for the treatment of rituximab refractory EBV-LPD after HCT. Data from these studies was presented at a clinical trials plenary session at the April 2015 AACR Annual Meeting and was subsequently updated at an oral presentation at the June 2015 American Society of Clinical Oncology, or ASCO, Annual Meeting.
In Study 95-024, patients with EBV-LPD following HCT were treated with EBV-CTL manufactured from T-cells derived from either the primary HCT donor or an unrelated third-party donor. The term primary HCT donor refers to the donor who provided hematopoietic stem cells for the HCT. A summary of results from these two studies is described below. The response rate, or RR, refers to the proportion of patients treated with EBV-CTL who had either a complete or partial response as best response to treatment when measured by radiographic imaging of the tumor. In a complete response, no visible
87
evidence of tumor following treatment was observed. In a partial response, the tumor was reduced in size by more than 50% but less than 100%. Disease control rate, or DCR, refers to the proportion of patients treated with EBV-CTL who had a complete response, a partial response, or stable disease following treatment. In stable disease the tumor could either have been reduced in size by less than 50% or could have increased in size by less than 50%.
Response Rate in EBV-LPD after HCT: Primary HCT Donor versus Third-party Donor Derived EBV-CTL
| EBV-CTL Source |
Number of Patients |
Prior Rituximab | Response Rate | Disease Control Rate |
||||||||||||
| Primary HCT Donor |
26 | 13 | 62 | % | 69 | % | ||||||||||
| Third-Party Donor(1) |
34 | 34 | 65 | % | 70 | % | ||||||||||
| (1) | Includes 22 patients from Study 11-130 plus 11 patients from Study 95-024 plus one patient treated under a treatment IND. |
The response rate and disease control rate in patients treated with primary donor derived EBV-CTL were 62% and 69%, respectively, as compared with 65% and 70%, respectively, in the combined group of patients treated with third party derived EBV-CTL. The similarity of these results suggests that the efficacy of treatment with primary donor derived and third-party donor derived EBV-CTL are comparable and that treatment with prior rituximab did not affect outcomes associated with the treatment. The similarity in efficacy observed following treatment with third party and primary donor derived EBV- CTL is important, as there are significant limitations associated with a therapy derived from the primary transplant donor. First, it can take approximately eight weeks to generate an EBV-CTL line from blood remaining from the primary HCT donor. In this amount of time and based on historical data, approximately half of those patients who had either failed to respond or who had relapsed after rituximab would likely have succumbed to their EBV-LPD and died before the cell line was available for therapeutic use. Second, due to the limited quantities of certain HCT donor materials such as umbilical cord blood, it is not possible to make a primary donor derived EBV-CTL line for all patients. Additionally, if the EBV-LPD is of host rather than donor origin, T-cells derived from the primary HCT donor may not be able to recognize this host tumor, and therefore would not be expected to be effective in combatting the disease. Thus, we believe that the availability of off-the-shelf third party derived EBV-CTL provides significant practical and therapeutic advantages in the treatment of rituximab refractory EBV-LPD. A median of two cycles of third party derived EBV-CTL were administered in these studies. In each cycle, three doses of EBV-CTL are given weekly for three weeks. In addition, a number of patients with disease located in the central nervous system, or CNS, responded to treatment with EBV-CTL suggesting that these cells are capable of passing through the blood-brain barrier.
The OS for patients with rituximab refractory EBV-LPD after HCT following treatment with third-party derived EBV-CTL was also presented by MSK at ASCO 2015. One-year and two-year OS were 56.3% and 46.9%, respectively, in the 12 patients from Study 95-024 and 71.8% and 63.8%, respectively, in the 22 patients from Study 11-130. MSK analyzed overall survival results using industry standard Kaplan-Meier, or K-M, methods. The K-M curves from Study 95-024 and 11-130 are depicted below and show the proportion of patients expected to be alive at different points in time, based on the results from the two studies. At one year in both studies and at 2 years in study 11-130, the K-M estimate of survival is greater than 50%, indicating that a median estimate of OS, or the time at which 50% of patients are expected to have died, had not yet been reached. In both studies, time zero for each patient is defined as the start of therapy with EBV-CTL.
88
Overall Survival: Rituximab Refractory Patients Treated with Third-Party Derived EBV-CTL
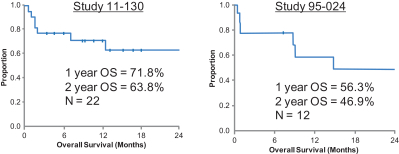
Although we expect that these K-M curves will evolve with ongoing follow-up of the patients and that a median OS may be reached in Study 11-130, we believe that these results compare favorably with the historically reported median survival of 16-56 days in the setting of rituximab failure. Moreover, patients who achieve a CR after EBV-CTL treatment have been noted by MSKCC to experience durable remissions without relapse.
89
The time course of a complete response following multiple cycles of EBV-CTL in a patient with rituximab refractory EBV-LPD is shown below using sequential positron emission tomography, or PET, scans. Also shown are the timing of rituximab and EBV-CTL therapy depicted by the corresponding set of arrows, the levels of EBV DNA in the blood as measured by EBV polymerase chain reaction, or EBV PCR, a sensitive and specific technique to detect viral DNA depicted in the corresponding line, as well as the levels of CTL precursors per milliliter of blood, or CTLp/ml, depicted in the corresponding line. CTLp/ml identifies and enumerates activated T-cells.
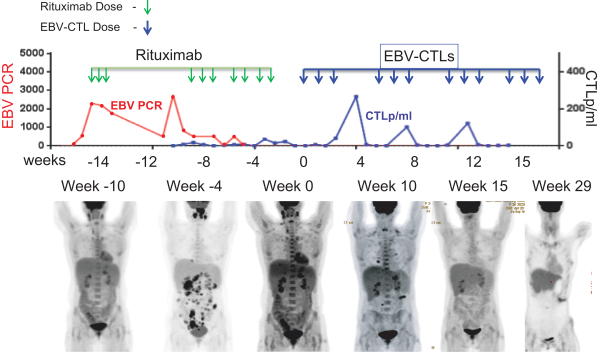
This patient developed EBV viremia, or high levels of virus in the blood, early post-HCT as noted in the line labeled EBV PCR. Her viremia responded to rituximab, but recurred and it again responded to a second cycle of rituximab. In the interim, she developed a rapidly progressive diffuse large B-cell lymphoma, or DLBCL, that was EBV positive. By week 0, defined as the start of EBV-CTL therapy, the lymphoma is visible in the lymph nodes as well as in the liver and spleen. She received a first cycle of third party EBV-CTL after which she had a partial response. The patient received three subsequent cycles of EBV-CTL after which she achieved a complete response. In conjunction with each cycle of EBV-CTL, expansion of EBV-specific cytotoxic T-cells was detected, as shown in the line labeled CTLp/ml. While these expansions were not durable, they mediated her complete response. The PET scans, in which dark areas correspond to areas of high metabolic activity, show both normal metabolism of organs such as the heart and abnormal metabolism in areas of lymphoma. After treatment with T-cells, the abnormal areas of metabolism recede, indicating eradication of tumor cells. In the final image, no abnormal metabolic activity is observed, reflecting a complete response to EBV-CTL therapy.
90
The ability to switch from one cell line to another led to the discovery of a hierarchy of HLA restriction. This is highlighted by the example below, in which a patient received three EBV-CTL lines (A, B and C) with different HLA restrictions, but only went into complete response upon administration of a fourth unique EBV-CTL line (D) with yet another HLA restriction. Future patients can be treated using an HLA selection algorithm based on the hierarchy elucidated in this manner that enables a more efficient choice of EBV-CTL.
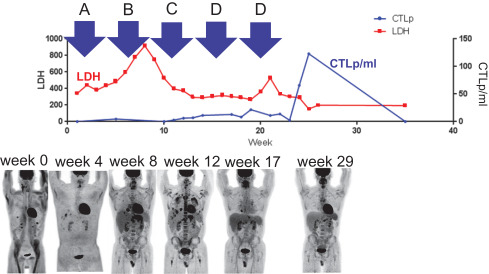
Across all patients enrolled in the two studies, reports of treatment related adverse events were low as reported at ASCO 2015. Seven possibly related grade 3 and two possibly related grade 4 adverse events were observed. One patient developed grade 1 skin GvHD responding to topical steroids with no systemic therapy required. No infusion related toxicities or cytokine release syndrome was observed.
In part due to these results, treatment with EBV-CTLs is recognized as a recommended treatment for persistent or progressive EBV-LPD as set forth in the 2015 National Comprehensive Cancer Network Guidelines. In addition, in December 2013, the FDA granted MSK cost reimbursement for use of the EBV-CTL in MSK’s clinical trials.
Since licensing our T-cell product candidates, the IND under which studies 95-024 and 11-130 were conducted has been transferred to us. We recently met with the FDA to discuss late-stage development to support a potential approval in this indication. Based on guidance from the FDA, we intend to conduct a pivotal study in rituximab-refractory EBV-LPD after HCT and expect to submit a special protocol assessment for this pivotal study. In addition, we had preliminary discussions with the FDA regarding late-stage development in the setting of rituximab-refractory EBV-LPD after SOT, and we will be incorporating this feedback into our subsequent development plans in this indication.
EBV-LPD after SOT
EBV-LPD after SOT, also referred to as post-transplant lymphoproliferative disease, or PTLD is a spectrum of lymphoid malignant disease associated with the use of immunosuppressive drugs after SOT. Patients with PTLD, one of the most common neoplastic diseases after SOT, commonly present with stage 3 or 4 disease. Reduction in immunosuppression, antiviral therapy, or surgical resection are common treatments, but many patients with PTLD require systemic therapy, especially those with aggressive lymphoma morphology such as DLBCL. Chemotherapy remains undesirable in PTLD because of myelotoxic side effects of cytotoxic therapy and associated infections and toxic deaths. In addition, recipients of chemotherapy face the prospect of secondary malignancies in the future. Rituximab with or without chemotherapy is often used off-label after reduction in immunosuppressive
91
therapy with a response rate of 44 to 60.5%. However, in the case of incomplete response to rituximab, historical data reported in the Annals of Hematology in 2007 show 33% OS at two years in patients with incomplete response to rituximab and 0% OS at two years in patients with high risk disease defined as those with age greater than or equal to 60 years, poor performance status, or elevated lactate dehydrogenase, or LDH. The rates of EBV-LPD after SOT vary by organ transplant type and degree of immunosuppression with rates in the audit and pediatric settings ranging from 1 to 10% in kidney transplants, 2 to 15% in liver transplants, 2 to 19.5% in heart transplants, 1.8 to 19.5% in lung transplants, 2.5-9.4% in heart/lung transplants, and 20-30% in bowel transplants. In addition, the rates of EBV-LPD after SOT appear to be higher in children than in adults. One of the unique features of EBV-LPD after SOT in comparison with the post-HCT setting is that the immunosuppression that ultimately gives rise to the lymphoma is in many cases required chronically and, as a result, the period of time during which an EBV-associated lymphoma may arise extends for the duration of immunosuppression. Although some cases of EBV-LPD in SOT occur within the first year, many occur years after transplant.
As reported at ASCO 2015, thirteen patients with EBV-LPD after SOT have been treated with third party derived EBV-CTL in studies 95-024 and 11-130. All patients had failed to respond to or relapsed following rituximab treatment; eleven SOT recipients also progressed after one to five courses of rituximab and chemotherapy. Six of the 11 patients who received chemotherapy had progressed after greater than or equal to three different chemotherapy regimens. Additionally, 12 of the 13 patients had high risk disease defined as those with age greater than or equal to 60 years, poor performance status, elevated LDH, or presence of disease in the central nervous system, or CNS. Response rate and OS results for these 13 patients as reported by MSK at ASCO 2015 were as follows.GTPs are FDA regulations and guidance documents that govern the methods used in, and the facilities and controls used for, the manufacture of human cells, tissues, and cellular and tissue based products, or HCT/Ps, which are human cells or tissue intended for implantation, transplant, infusion, or transfer into a human recipient. The primary intent of the GTP requirements is to ensure that cell and tissue based products are manufactured in a manner designed to prevent the introduction, transmission and spread of communicable disease. FDA regulations also require tissue establishments to register and list their HCT/Ps with the FDA and, when applicable, to evaluate donors through screening and testing.
Response Rate in EBV-LPD after SOT: Third-Party Donor Derived EBV-CTL
| EBV-CTL Source |
Number of Patients |
Prior Rituximab | Prior Chemotherapy |
Response Rate | ||||||||||||
| Third-Party Donor |
13 | 13 | 11 | 62 | % | |||||||||||
The response rate observed in the rituximab refractory post SOT setting of 62% is similar to the response rates observed in the post HCT setting. The responses observed were also durable with one durable CR (>22mo) and seven durable PRs (range: 6-114 months) in heavily pre-treated patients. No patient with a CR or PR has had progression requiring alternative therapy.
OS in EBV-LPD after SOT: Third-party Donor Derived EBV-CTL
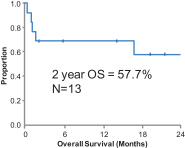
92
The two-year OS observed in the post SOT setting was 57.7% indicating that a median OS had not yet been reached. Although we expect that these K-M curves will evolve with ongoing follow-up of the patients and that a median OS may be reached, we believe that these results compare favorably with the historically reported median OS of 33% at two years in the setting of incomplete response to rituximab and 0% at 2 years in the setting of high-risk disease.
Based on this data, we plan to meet with the regulatory authorities to solicit agreement on the plan for late-phase development to support a potential marketing approval for EBV-CTL in the treatment of EBV-LPD after SOT.
Other EBV Associated Diseases
In immunocompetent patients, EBV-associated malignancies include: Burkitt’s lymphoma, Hodgkin lymphoma, non-Hodgkin lymphoma such as DLBCL, or NHL, NK T-cell lymphomas, nasopharyngeal carcinoma, and gastric cancer. Typically, these malignancies occur many years after primary EBV infection. For Burkitt’s lymphoma, approximately 15-30% of cases are associated with EBV in the US and EU. For Hodgkin lymphoma, approximately 20-50% of cases are associated with EBV in the US and EU; however, many of these are responsive to chemotherapy. Approximately 10% of include T-cell lymphoproliferative disorders and nearly 100% of T/NK cell lymphomas are associated with EBV. In nasopharyngeal carcinoma, or NPC, the association with EBV is such that regardless of geography nearly 100% of the nonkeratinising tumors and all the tumor cells have been demonstrated to be monoclonally EBV-positive. EBV-positive gastric cancers, or GCs, make up approximately 10% of all GCs. In some of these tumor types, multiple EBV proteins are associated with the disease and in others, a smaller subset are made.
In the setting of CNS disease, a number of observations implicate EBV in the pathogenesis of multiple sclerosis. For example, MS patients are universally EBV seropositive, there are high levels of anti-EBV antibodies, their T-cells have altered immune function, there is an increase in spontaneous EBV-induced peripheral blood B-cell transformation, there is increased shedding of EBV from saliva, and EBV infected B-cells and plasma cells accumulate in the brain.
We intend to explore the therapeutic utility of EBV-targeted cellular therapy in a number of these tumor types. In order to improve efficacy in some of these patient populations, we expect to develop specific cellular therapies that target the precise EBV antigen implicated in a disease. As we expand the use of EBV-CTL in these settings, we expect to present data at major scientific meetings and engage regulatory authorities to solicit agreement on the plan for late-phase development to support a marketing approval for EBV-CTL in the treatment of certain of these conditions.
CMV Targeted T-cells for CMV Infection and Other CMV Associated Malignancies
CMV, also known as HHV-5, is a member of the Herpes virus family. CMV infection rate gradually increases throughout childhood, and, once infected, an individual carries the virus for life due to the ability of CMV to establish a latent state of infection. It is estimated that CMV infection affects 50-90% of the global adult population. Immunocompromised patients, including HCT and SOT patients, human immunodeficiency, or HIV, patients, and to a lesser extent cancer patients, are at highest risk for developing significant disease syndromes caused by CMV, including interstitial pneumonia, gastrointestinal infection, central nervous system disease, hepatitis, retinitis, and encephalitis. CMV reactivations have also been reported to occur frequently in critically ill immunocompetent patients and are associated with prolonged hospitalization or death. Congenital CMV infection causes an estimated 400 deaths per year and leaves approximately 8,000 children per year with permanent disabilities such as hearing loss, vision loss, or mental retardation in the United States.
93
In the oncology setting, CMV is commonly associated with glioblastoma multiforme, or GBM, where approximately 95% of these tumors express CMV. In GBM, multiple CMV proteins are associated with the disease.
While there have been many advances in detecting and managing CMV infections, the virus continues to be one of the most important infectious diseases among immunocompromised patients. Antiviral drugs in the form of prophylaxis or preemptive treatment strategies have reduced morbidity and mortality, though adverse effects such as neutropenia and toxicity remain a challenge. The emergence of resistance to antiviral drugs also presents challenges to laboratory medicine and patient care.
The estimated number of patients per year in the United States and European Union with refractory CMV infection and associated malignancies is highlighted in the figure below.
| Indication |
Estimated Number of Patients |
|||
| Anti-viral resistant CMV after HCT |
2,000 | |||
| Anti-viral resistant CMV after SOT |
1,300 | |||
| Anti-viral resistant, HIV associated CMV retinitis |
500 | |||
| Glioblastoma multiforme |
21,000 | |||
| Congenital CMV |
12,500 | |||
CMV Viremia and Disease after HCT
Despite the use of prophylactic and preemptive therapy using small molecule antivirals, many post-HCT patients progress to developing overt, symptomatic CMV viral diseases such as retinal infections that risk permanent blindness, encephalopathy with the risk of permanent brain damage and other serious morbidities. In prophylactic therapy, immunocompromised patients are given antiviral drugs for several months after HCT. In preemptive therapy, patients are intensively monitored for CMV activity using sensitive laboratory methods, and short-term antiviral treatment is given only to those with significant viral counts (CMV viremia) before symptoms and overt CMV disease occur. However, the antiviral drugs used to treat CMV have significant toxicities, including marrow toxicity for ganciclovir, valganciclovir and cidofovir, and renal toxicity for foscarnet and cidofovir. In addition, CMV drug resistance mutations arise during this antiviral therapy.
94
MSK has conducted one Phase 1 clinical study and two Phase 2 clinical trials of CMV-CTL that included patients with CMV viremia and CMV disease, in each case resistant to antiviral drug treatment. An interim summary of MSK’s clinical experience was reported at the December 2014 ASH Annual Meeting. This analysis evaluated outcomes in 38 patients who were treated with CMV-CTLs after failing a median of 113 days of prior antiviral therapy with a median of four different antiviral drugs. Following the ASH presentation, in January 2015, MSK provided us with a more current summary of its clinical experience to date to account for additional cycles of CMV-CTL therapy in which certain patients with stable disease and partial responses from the interim summary had converted to complete responses after additional CMV-CTL therapy. The results from MSK’s updated summary are reported in the table below:
| CMV Treatment Setting |
Number of Patients Treated |
Number
of Patients Evaluable(3) |
Overall Response Rate (%) | |||||||
| Antiviral resistant CMV Viremia(1) |
26 | 25 | 64% 9 complete responses 7 partial responses | |||||||
| Antiviral resistant CMV Disease(2) |
12 | 9 | 67% 5 complete responses 1 partial response | |||||||
| (1) | Responses in patients treated for viremia alone with CMV-CTLs were considered to be complete responses if the viremia resolved completely and partial responses if the viral load fell 100-fold or more. |
| (2) | Responses in patients treated for overt disease were considered to be complete responses if all detectable CMV viremia and disease resolved and partial responses if patients became asymptomatic. |
| (3) | Four patients were not evaluable due to receipt of confounding concomitant antiviral medications (n=2), concomitant high dose steroids (n=1)and withdrawal of consent (n=1). |
We believe this data suggests a high response rate among patients with otherwise refractory CMV viremia and disease. Overall, CMV-CTL therapy was well tolerated and no patients developed de novo GvHD, or a flare-up of prior GvHD, in association with infusion of CMV-CTLs.
95
Two individual patient experiences following treatment with CMV-CTL are described below. The graph below shows the time course of a reduction in CMV viremia and a reciprocal increase in the proliferation of CMV-CTL following administration. The improvement in CMV viremia is evidenced by a decline in blood CMV DNA ascertained by CMV PCR. The reciprocal proliferation of CMV-CTL following administration is reflected by the release of interferon-gamma (IFNg[+]) in CMV-CTL detected via flow cytometry; interferon-gamma positivity identifies and enumerates activated T-cells.
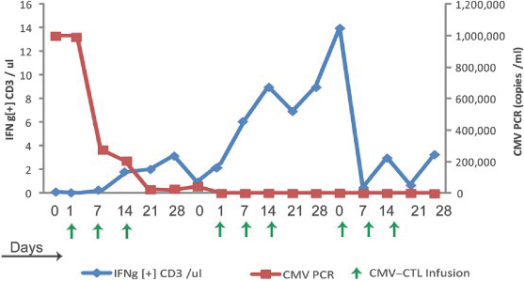
The following retinal photographs depict improvement in CMV retinitis for a patient treated with CMV-CTL. The baseline images, labeled “a” and “b”, show the right and left retinae, respectively, at the start of CMV-CTL administration. Subsequent images “c” and “d” capture the response of the patient’s CMV retinitis at six weeks after first CMV-CTL administration. In the retinal images, the dark areas correspond to affected portions of the retina. The response of retinal disease to treatment with CMV-CTL suggests that, as was observed with EBV-CTL, the cells are able to reach areas of the body typically not accessible to systemic therapies.
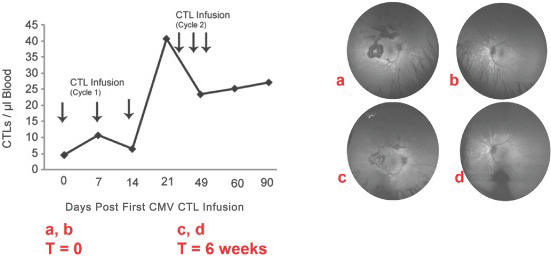
96
Other CMV Associated Conditions and Malignancies
CMV is among the most common and important infectious agents among SOT patients. In transplant recipients, the factor that most strongly influences the degree of morbidity and mortality caused by CMV is the type and extent of immunosuppressive therapy. Reactivation can occur in any individual who is latently infected. However, no transplant patient is safe from CMV since this pathogen can also be acquired from the transplanted organ. CMV can also be community acquired following transplantation and is of particular concern in pediatric transplant patients. In SOT patients, particularly those who develop a primary infection during the first three months post-transplant, a specific CMV syndrome consisting of fever, malaise, arthralgia, and neutropenia may be observed. CMV infections have been associated with indirect effects, such as dysfunction or rejection of the transplanted organ; increased risk for bacterial or fungal opportunistic infections; development of EBV associated post-transplant lymphoproliferative disease; accelerated atherosclerosis in heart transplant patients; and decreased patient and graft survival. In the absence of antiviral intervention, symptomatic CMV infections occur in approximately: 39 to 41% of heart-lung transplant recipients, 9 to 35% of heart transplant recipients, 22 to 29% of liver and pancreas transplant recipients, 8 to 32% of kidney transplant recipients, 50% of kidney-pancreas transplant recipients; and 22% of small-bowel transplant recipients.
CMV infection is one of the most frequently occurring opportunistic infections in AIDS patients. The advent of highly active antiretroviral therapy, or HAART, has resulted in an 80% decrease in the incidence of CMV retinitis, which previously affected an estimated 30% of AIDS patients. However, some patients do not have access or respond well to HAART. Thus, CMV still remains a concern in patients when CD4+ T-cell counts decline to 50 to 100 cells per microliter.
In the last few years, multiple investigators have confirmed the presence of CMV in GBM, and multiple CMV gene products are now implicated in biologically relevant GBM signaling pathways. Preclinical studies published in 2013 in the journal Cancer Research indicate that CMV may be unique in its ability to promote oncogenesis in the setting of a prior tumor suppressor dysfunction. Malignant gliomas are the most common primary central nervous system, or CNS, neoplasms in humans. However, most patients who are diagnosed with a glioblastoma multiforme which is the most common and malignant form of malignant glioma, still have a mean survival less than two years. Given the emerging role of CMV in GBM, antiviral strategies that block CMV expression or stimulate immune attack of CMV-infected cells may prove beneficial as novel therapeutics for GBM, and both direct antiviral strategies and specific CMV-based immunotherapy approaches are showing early promise.
Based on the established proof of concept for CMV-CTL in the treatment of antiviral resistant CMV viremia and disease after HCT, we intend to explore the therapeutic utility of CMV-CTL in a number of other immunocompromised states, including potentially after SOT and in the setting of CMV-associated retinitis. In addition, the clinical data with both EBV-CTL and CMV-CTL has demonstrated the ability of these product candidates to access the brain and mediate clinical responses in difficult to treat CNS disease. As a result, we believe that CMV-targeted cellular therapy may provide a novel off-the-shelf cellular therapeutic option for patients with GBM, and we intend to explore its clinical utility in this setting as well in conjunction with the development of CMV-targeted cellular therapy that target the precise CMV antigen implicated in the disease.
As we expand the use of CMV-CTL in these settings, we expect to present data at major scientific meetings and engage regulatory authorities to solicit agreement on the plan for late-phase development to support potential marketing approval for EBV-CTL in the treatment of certain of these conditions.
WT1 Targeted T-Cells for Hematologic Malignancies and Solid Tumors
WT-1 is an intracellular protein that is overexpressed in a number of cancers, including acute myeloid leukemia, or AML, multiple myeloma, or MM, and non-small cell lung, breast, pancreatic,
97
ovarian, and colorectal cancers. We have two ongoing Phase 1 studies sponsored and conducted by MSK with primary HCT donor derived WT1-CTL. The first is a dose escalation trial of WT1-CTL for residual or relapsed leukemia after HCT. The second is a dose escalation trial of WT1-CTL following T-cell depleted HCT for patients with relapsed or refractory MM. As these studies complete, we expect our collaborating investigators at MSK to present data at upcoming conferences. In addition, based on data from these studies, we expect to explore the clinical utility of WT1-CTL in these hematologic malignancies. In the setting of solid tumors, we believe that treatment with WT1-CTL may be potentiated through combination approaches with other agents. Therefore, we plan to embark on a number of combination studies in these indications.
Additional Platform Expansion Activities
We anticipate that our T-cell technology platform will have utility beyond the current set of targets to which it has been directed. We and MSK have agreed to collaborate on further research to develop additional cellular therapies, which may include T-cell programs targeted against other antigens and chimeric antigen receptor, or CAR-T cell programs, and which we have an option to license. For example, we may develop cellular therapies with MSK or others directed towards other viral targets, such as HPV, which is associated with cervical cancer, anal cancer, head and neck cancer and JCV, which causes progressive multifocal leukoencephalopathy and is associated with a subset of solid tumors. We believe that viral antigens are well suited to adoptive immunotherapy given that people with normal immune systems are able to mount robust responses to these viral targets, but immunocompromised patients and some cancer patients are not. We also intend to license or acquire additional product candidates or technologies to enhance our existing T-cell technology platform.
Competition
The biotechnology and pharmaceutical industries are characterized by rapidly advancing technologies, intense competition and a strong emphasis on proprietary products. While we believe that our innovative technology, knowledge, experience and scientific resources provide us with competitive advantages, we face potential competition from many different sources, including major pharmaceutical, specialty pharmaceutical and biotechnology companies, academic institutions and public and private research institutions. Some of these potential competitors may have a more established presence in the market and significantly greater financial, technical and human resources than we have. Our commercial opportunity will be reduced or eliminated if our competitors develop and commercialize products that are safer, more effective, have fewer side effects or are less expensive than any products that we may develop.
If approved, PINTA 745 or STM 434 would compete with currently marketed drugs and therapies used for treatment of the following indications, and potentially with drug candidates currently in development for the same indications:
Muscle Wasting-Related Indications
There currently are no FDA or European Medicines Agency, or EMA, approved products for the treatment of PEW in dialysis patients and we are not aware of any product candidates in clinical development for this indication. However, products are currently marketed or used off-label for the muscle wasting-related indication for which we are developing PINTA 745, and a number of companies are or may be developing new treatments for muscle wasting indications. The current treatment for PEW and cancer cachexia often involves the administration of readily available nutritional supplements and appetite stimulants including, in some jurisdictions, marijuana. In addition, there are two commercially available steroids, nandrolone and oxandrolone, that are sometimes prescribed off-label for the treatment of weight loss in cancer patients.
98
Additionally, a number of companies are developing drug candidates for muscle wasting applications, including: Eli Lilly & Co., which is conducting Phase 1 clinical studies and Phase 2 clinical trials for LY2495655, and Pfizer Inc., which is conducting Phase 1 clinical studies for PF-06252616, both of which are myostatin antibodies, to evaluate their ability to increase and improve muscle mass in various patient populations; Novartis Corporation, which is conducting Phase 1 clinical studies and Phase 2 clinical trials for BYM338, an ActR2B antibody, to evaluate its ability to build muscle in patients with various muscle-wasting conditions; Ligand Pharmaceuticals, which is developing LGD-4033, a selective androgen receptor modulator, for muscle wasting; Regeneron Pharmaceuticals, Inc., which is developing REGN1033, a myostatin antibody, in collaboration with Sanofi-Aventis for sarcopenia; Acceleron Pharma, which is developing ACE-083, a modified cysteine knot ligand trap of the TGF-ß superfamily, for diseases in which improved muscle strength may provide a clinical benefit, such as inclusion body myositis and certain forms of muscular dystrophy; and GTx, Inc., which is developing ostarine, a selective androgen receptor modulator for cachexia.
Ovarian Cancer
There are numerous approved products and therapies for ovarian cancer, and a number of companies are or may be developing new treatments for ovarian cancer and other solid tumors. These therapies, as well as promotional efforts by competitors and clinical trial results of competitive products, could significantly diminish any ability to market and sell STM 434. Approved drug therapies for ovarian cancer include: chemotherapy with platinum compounds such as cisplatin or carboplatin and taxane compounds such as paclitaxel or docetaxel; bevacizumab in combination with chemotherapy compound such as liposomal, doxorubicin, paclitaxel or topotecan; olaparib in patients with deleterious or suspected deleterious germline BRCA mutated advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy; and hormone therapies including goserelin, leuprolide, tamoxifen, letrozole, anastrozole and exemestane.
We are aware of other companies engaged in clinical development of compounds for treatment of ovarian cancer. These include:
| • | PARP inhibitors such as Tesaro’s niraparib; |
| • | angiogenesis inhibitors, such as Genentech/Roche’s bevacizumab (Avastin); |
| • | VEGFr tyrosine kinase inhibitors such as Boehringer Ingelheim GmbH’s nintedanib and AstraZeneca plc’s recentin; |
| • | selective 17,20-lyase inhibitors such as Takeda Pharmaceutical’s TAK-700; |
| • | anti-folates such as Eisai’s farletuzumab; and |
| • | other therapies in development, including those from GlaxoSmithKline plc, Amgen and Clovis Oncology, |
however, there are no targeted therapies approved by the FDA or EMA for the treatment of ovarian cancer that address the underlying biology.
T-Cell Product Candidates
Should our T-cell product candidates be approved for use, we will face substantial competition. In addition to the current standard of care for patients, commercial and academic clinical trials are being pursued by a number of parties in the field of immunotherapy. Early results from these trials have fueled continued interest in immunotherapy. In addition, if approved, the MSK T-cell programs would compete with currently marketed drugs and therapies used for treatment of the following indications, and potentially with drug candidates currently in development for the same indications:
99
EBV-LPD
There currently are no FDA or EMA approved products for the treatment of EBV-LPD. However, some approved products and therapies are currently used off-label in this setting, and a number of companies and academic institutions that may license therapies to companies in the future are or may be developing new treatments. These therapies, as well as promotional efforts by competitors and clinical trial results of competitive products, could significantly diminish any ability to market and sell EBV-CTL. The current treatment for EBV-LPD involves administration of rituximab as a single agent or in the SOT setting, in combination with chemotherapy regimens. Additionally, a number of companies and academic institutions are developing drug candidates for EBV-LPD, including: Cell Medica Ltd., or Cell Medica, which is conducting Phase 2 clinical studies for Cytorex EBV, an autologous EBV specific T-cell therapy, in NK/T-cell lymphoma, Adcyte LLC, or Adcyte, which has licensed multi-virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor, and ViraCyte, which has licensed virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor.
CMV Infection
There are numerous approved products and therapies for the treatment of CMV infection, and a number of companies and academic institutions that may license therapies to companies in the future are or may be developing new treatments for CMV infection. These therapies, as well as promotional efforts by competitors and clinical trial results of competitive products, could significantly diminish any ability to market and sell the CMV targeted T-cell therapy from MSK. Drug therapies approved or commonly used for CMV infection include antiviral compounds such as ganciclovir, valganciclovir, cidofovir or foscarnet.
Additionally, a number of companies and academic institutions are developing drug candidates for CMV infection, including: Shire plc, or Shire, which is conducting Phase 2 clinical trials of maribavir, a UL97 protein kinase inhibitor; Merck & Co., Inc., or Merck, which is conducting Phase 3 clinical trials of letermovir, a CMV terminase inhibitor; Chimerix, Inc., or Chimerix, which is conducting Phase 3 clinical trials for brincidofovir, a lipid conjugated nucleotide analogue of cidofovir; Cell Medica, which is conducting Phase 3 clinical trials for Cytovir CMV, a CMV-specific cell therapy product derived from primary HCT transplant donors which is also marketed in the UK under a “Specials” license; Adcyte, which has licensed multi-virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor, and ViraCyte, which has licensed virus specific T-cells from Baylor University that are currently in clinical trials sponsored by Baylor.
License Agreements
License for PINTA 745
In September 2012, we entered into a license agreement with Amgen under which Amgen granted us an exclusive license under certain Amgen patent rights and regulatory filings, and a non-exclusive license under certain Amgen know-how, to develop and commercialize throughout the world, excluding Japan, products comprising Amgen’s proprietary compound known as AMG 745, which we now refer to as PINTA 745. We have the right, subject to certain limitations, to grant sublicenses under such licensed intellectual property, in connection with licensing the licensed product. Our exclusive rights are subject to a prior license granted by Amgen to Takeda to the licensed patent rights exclusively in Japan.
Under this agreement, we are responsible for developing and commercializing the licensed product, at our cost, are required to use commercially reasonable efforts with respect to such development and commercialization activities, and must meet specific diligence obligations. We paid
100
Amgen an upfront license fee of $250,000, issued 205,128 shares of Series A-1 convertible preferred stock, and made $553,000 in payments to date to Amgen for purchases of clinical supplies. Each of the 205,128 shares of Series A-1 convertible preferred stock converted into one share of common stock upon the closing of our initial public offering. We are obligated to make payments to Amgen upon receipt of certain clinical supplies from Amgen, upon the achievement of certain development and commercialization milestones of up to $129.0 million, as well as escalating mid to high single-digit royalties based on sales of the licensed products by us, our affiliates or our sublicensees. We hold the first right to file, prosecute, maintain and enforce all licensed rights throughout the world, except in Japan, where Amgen has the sole right to do so, and Amgen retains certain step-in rights.
This agreement, unless terminated earlier, will continue on a country-by-country basis until the expiration of the last to expire of all royalty obligations we owe to Amgen, which will occur on the later of (a) the date on which exploitation of a licensed product is no longer covered by a valid claim of a patent under the agreement which covers a product in an applicable country, (b) the loss of regulatory exclusivity in such country or (c) 10 years after the first commercial sale of the applicable licensed product in such country. Upon expiration of the agreement, we retain non-exclusive rights to the licensed Amgen intellectual property. Amgen may terminate the agreement if we materially breach the agreement and do not cure such breach in a specified notice period, for a failure of our specified diligence obligations, if we experience certain insolvency events, or if we or our sublicensee challenge the patentability, validity or enforceability of any of the Amgen patents licensed under the agreement. We may terminate the agreement for Amgen’s uncured material breach, or if our board of directors concludes that, due to safety, efficacy, marketability, patent coverage or competition concerns, the development or commercialization of a licensed product is no longer commercially practicable for us.
Other Amgen License Agreements
In September 2012, we entered into two other license agreements with Amgen under which Amgen granted us worldwide exclusive licenses under certain Amgen patent rights and regulatory filings, and non-exclusive licenses under certain Amgen know-how, to develop and commercialize products comprising certain of Amgen’s proprietary compounds known as AMG 777, AMG 434, AMG 217, ActR2B5, AMG 842 and M43. We now refer to AMG 777 as ATA 777, AMG 434 as STM 434, AMG 217 as STM 217 and AMG 842 as ATA 842. We have the right, subject to certain limitations, to grant sublicenses under such licensed intellectual property, in connection with licensing the covered products.
Under both of these license agreements, we are responsible for the worldwide development and commercialization of the licensed products, at our cost, are required to use commercially reasonable efforts with respect to such development and commercialization activities, and must meet certain specific diligence obligations. In exchange for these licenses, we issued 410,256 shares of Series A-1 convertible preferred stock. Each of the 410,256 shares of Series A-1 convertible preferred stock converted into one share of common stock immediately prior to completion of our initial public offering. We are obligated to make payments to Amgen upon the achievement of certain development and commercialization milestones totaling up to $81.5 million for each license agreement, as well as escalating low to mid single-digit royalties based on sales of the licensed products by us, our affiliates or our sublicensees. We hold the first right to file, prosecute, maintain and enforce all licensed rights under these licenses throughout the world, and Amgen retains certain step-in rights.
Both license agreements with Amgen, unless terminated earlier, will continue on a country-by-country basis until the expiration of the last to expire of all royalty obligations we owe to Amgen, which will occur on the later of (a) the date on which exploitation of a licensed product is no longer covered by a valid claim of a patent under the agreement which covers the product in an applicable country, (b) the loss of regulatory exclusivity in such country or (c) 10 years after the first commercial sale of the
101
applicable licensed product in such country. Upon expiration of each agreement, we retain non-exclusive rights to the relevant licensed Amgen intellectual property. Amgen may terminate either agreement if we materially breach the agreement and do not cure such breach in a specified notice period, for a failure of our specified diligence obligations, if we experience certain insolvency events, or if we or our sublicensee challenge the patentability, validity or enforceability of any of the Amgen patents licensed under the applicable agreement. We may terminate each agreement for Amgen’s uncured material breach, or if our board of directors concludes that, due to safety, efficacy, marketability, patent coverage or competition concerns, the development or commercialization of the relevant licensed product is no longer commercially practicable for us.
MSK Option and License Agreement
In September 2014, we entered into an exclusive option agreement with MSK under which we acquired the right to exclusively license from MSK the worldwide rights to three clinical stage T-cell programs. The initial option period was for 12 months. In exchange for the exclusive option, we paid MSK $1.25 million in cash and issued 59,761 shares of our common stock to MSK. We and MSK also agreed to collaborate on further research to develop additional cellular therapies, which may include T-cell programs targeted against other antigens and/or CAR-T, and which we also would hold an option to license, if developed.
In June 2015, we exercised the option and entered into a license agreement with MSK. Under the terms of the license agreement, MSK granted us a worldwide, exclusive license under certain patent rights, know-how and a library of T-cells and cell lines, to research, develop, manufacture and commercialize T-cell products specific to CMV, EBV or WT1 that comprise or are based on or made using such licensed rights. MSK also agreed to transfer certain INDs related to the licensed products to us. We have agreed to use commercially reasonable efforts to commercialize the licensed products and, if commercialized, continue active marketing efforts for any commercialized licensed product through the term of the license agreement.
In connection with the option exercise and the execution of the license agreement, we will make an upfront cash payment to MSK of $4.5 million. We are obligated to make additional milestone payments of up to $33.0 million with respect to the three licensed clinical stage T-cell programs based on achievement of specified development, regulatory and sales-related milestones. We are also required to make escalating mid to high single-digit royalty payments to MSK based on sales of any licensed products. In addition, under certain circumstances, we must make certain minimum annual royalty payments to MSK, which are creditable against earned royalties owed for the same annual period. We are also obligated to pay a low double-digit percentage of consideration we receive for sublicensing the licensed rights.
The license agreement expires for each licensed T-cell product on a licensed product-by-licensed product basis and a country-by-country basis, on the latest of: (i) expiration of the last licensed patent rights related to such licensed product in such country, (ii) expiration of any market exclusivity period granted by law with respect to such licensed product in such country, and (iii) a specified number of years after the first commercial sale of the licensed product in such country. Upon expiration of the license agreement, the licenses granted to us will become non-exclusive royalty-free, perpetual and irrevocable. MSK may terminate the license agreement if we materially breach the agreement and does not cure such breach within a specified period or if we experience certain insolvency events.
102
Intellectual Property
Patents
Our commercial success depends in part on our ability to obtain and maintain proprietary protection for our product candidates, to operate without infringing on the proprietary rights of others and to prevent others from infringing our proprietary rights. Our policy is to seek to protect our proprietary position by, among other methods, filing US and non-US patent applications related to our proprietary technology, inventions and improvements that are important to the development and implementation of our business. We also rely on trade secrets, know-how, continuing technological innovation and potential in-licensing opportunities to develop and maintain our proprietary position. Additionally, we expect to benefit from a variety of statutory frameworks in the United States, Europe and other countries that relate to the regulation of biosimilar molecules and orphan drug status. These statutory frameworks provide certain periods of regulatory exclusivity for qualifying molecules. See “Government Regulation.”
We seek composition-of-matter and method-of-treatment patents for each of our product candidates in key therapeutic areas.
Our in-licensed and proprietary patent estate, on a worldwide basis, includes approximately 148 issued patents, six allowed applications and 203 pending patent applications, with certain of these pending and issued claims relating to PINTA 745 and STM 434. These figures include in-licensed patents and patent applications to which we generally hold exclusive commercial rights.
Individual patents extend for varying periods of time depending on the date of filing of the patent application, the priority date claimed and the legal term of patents as determined by the applicable law in the countries in which those patents are obtained.
Generally, patents issued from applications filed in the United States are effective for 20 years from the earliest non-provisional filing date. In addition, in certain instances, a patent term can be extended to recapture a portion of the term effectively lost as a result of the FDA regulatory review period; however, the restoration period cannot be longer than five years and the total patent term including the restoration period must not exceed 14 years following FDA approval. The duration of non-US patents varies in accordance with provisions of applicable local law, but typically, a patent’s life is 20 years from the earliest international filing date. Our licensed, issued US patents are expected to expire on dates ranging from 2027 to 2029, and our licensed issued non-US patents are expected to expire on dates ranging from 2023 to 2029, exclusive of possible patent term extensions. Our pending owned and licensed applications with respect to our product candidates, if issued, are expected to expire, as to applications filed in the United States, on dates ranging from 2023 to 2035, and, as to applications filed in jurisdictions outside the United States, on dates ranging from 2023 to 2035, exclusive of possible patent term extensions or adjustments. However, the actual protection afforded by a patent varies on a product- by-product basis, from country to country and depends upon many factors, including the type of patent, the scope of its coverage, the availability of extensions of patent term, the availability of legal remedies in a particular country and the validity and enforceability of the patent.
National and international patent laws concerning protein-based biologics such as our products remain highly unsettled. No consistent policy regarding the patent-eligibility or the breadth of claims allowed in such patents has emerged to date in the United States, Europe or other countries. Changes in either the patent laws or in interpretations of patent laws in the United States and other countries can diminish our ability to protect our inventions and enforce our intellectual property rights. Accordingly, we cannot predict the breadth or enforceability of claims that may be granted in our patents or in third-party patents. The biotechnology and pharmaceutical industries are characterized by extensive
103
intellectual property litigation. Our ability to maintain and solidify our proprietary position for our product candidates and technology will depend on our success in obtaining effective claims for any patent and enforcing those claims once a patent is granted. We do not know whether any of the patent applications that we may file or license from third parties will result in the issuance of any patents. The issued patents that we own or may receive in the future may be challenged, invalidated or circumvented, and the rights granted under any issued patents may not provide us with sufficient protection or competitive advantages against competitors with similar technology. Furthermore, our competitors may independently develop and commercialize similar drugs or duplicate our technology, business model or strategy without infringing our patents. Because of the extensive time required for clinical development and regulatory review of any drug we may develop from our product candidates, it is possible that, before any of our drugs can be commercialized, any related patent may expire or remain in force for only a short period following commercialization, thereby reducing any advantage of any such patent. The patent positions for our two lead molecularly targeted product candidates T-cell product candidates are summarized below:
PINTA 745 Patent Portfolio
We hold exclusive rights to five issued US patents directed to PINTA 745 relating to composition-of-matter and related methods of use claims, one issued European patent (registered in most countries of the European Patent Convention) and additional issued patents or pending patent applications in many jurisdictions worldwide, including the US, the European Patent Office, Argentina, Australia, Brazil, Canada, China, Egypt, Israel, Japan, the Republic of Korea, Malta, Mexico, Norway, New Zealand, Poland, Serbia, Singapore, Thailand, Taiwan, South Africa, Kosovo, Hong Kong, the Philippines, and Eurasia (validated in Russia). The expected expiration dates for these patents and patent applications range from 2023 to 2035, exclusive of possible patent term extensions or adjustments.
STM 434 Patent Portfolio
We hold exclusive rights to four issued US patents directed to STM 434 relating to composition-of-matter and related methods of use claims, and issued patents or pending patent applications related to STM 434 in many jurisdictions worldwide, including in the US, Argentina, Australia, Brazil, Botswana, Canada, Chile, China, Colombia, Costa Rica, Algeria, the Eurasian Patent Office, Egypt, the European Patent Office, the Gulf Cooperation Council, Hong Kong, Indonesia, Israel, India, Jordan, Japan, the Republic of Korea, Libya, Morocco, Mexico, Malaysia, New Zealand, Peru, the Philippines, Singapore, Tunisia, Taiwan, Ukraine, Vietnam, and South Africa. The expected expiration dates for these patents and patent applications range from 2026 to 2035, exclusive of possible patent term extensions or adjustments.
T-cell Technology Patent Portfolio
We hold exclusive rights to one pending US provisional patent application directed to EBV-CTL methods of use claims, one pending US provisional patent application directed to methods of identifying and selecting third-party, donor derived targeted T-cell lines for therapeutic use and two pending US provisional patent applications directed to CMV-CTL method of use claims. The United States patent system permits the filing of provisional and non-provisional patent applications. A provisional patent application is not examined for patentability by the United States Patent and Trademark Office, or USPTO, and automatically expires 12 months after its filing date. As a result, a provisional patent application cannot mature into a patent. Provisional patent applications are often used, among other things, to establish an early effective filing date for a later-filed non-provisional patent application. A non-provisional patent application is examined by the USPTO and can mature into a patent once the USPTO determines that the claimed invention meets the standards for patentability.
104
Trade Secrets
In addition to patents, we rely upon unpatented trade secrets and know-how and continuing technological innovation to develop and maintain our competitive position. We seek to protect our proprietary information, in part, using confidentiality agreements with our commercial partners, collaborators, employees and consultants and invention assignment agreements with our employees. These agreements are designed to protect our proprietary information and, in the case of the invention assignment agreements, to grant us ownership of technologies that are developed through a relationship with a third party. These agreements may be breached, and we may not have adequate remedies for any such breach or any unauthorized disclosure of our proprietary information. In addition, our trade secrets may otherwise become known or be independently discovered by competitors. To the extent that our commercial partners, collaborators, employees and consultants use intellectual property owned by others in their work for us, disputes may arise as to the rights in related or resulting know-how and inventions.
Government Regulation
Overview of US Government Regulation
The preclinical studies and clinical testing, manufacture, labeling, storage, recordkeeping, advertising, promotion, export, marketing and sales, among other things, of our product candidates are subject to extensive regulation by governmental authorities in the United States and other countries. In the United States, pharmaceutical products are regulated by the FDA under the Federal Food, Drug, and Cosmetic Act and other laws, including, in the case of biologics, the Public Health Service Act. We expect PINTA 745 and STM 434 to be regulated by the FDA as biologics and to be reviewed by the Center for Drug Evaluation and Research as proteins intended for therapeutic use. Protein therapeutics require the submission of a biologics license application, or BLA, and approval by the FDA prior to being marketed in the US. Manufacturers of protein therapeutics may also be subject to state regulation. Our T-cell product candidates, including EBV-CTL and CMV-CTL, are regulated by the FDA as biologics, and to be reviewed by the Center for Biological Evaluation and Research, and will require the submission of BLAs and approval by the FDA prior to being marketed in the US. Failure to comply with FDA requirements, both before and after product approval, may subject us or our partners, contract manufacturers, and suppliers to administrative or judicial sanctions, including FDA refusal to approve applications, warning letters, product recalls, product seizures, total or partial suspension of production or distribution, fines and/or criminal prosecution.
The steps required before a biologic may be approved for marketing of an indication in the United States generally include:
| • | completion of preclinical laboratory tests, animal studies and formulation studies conducted according to good laboratory practices, or GLPs, and other applicable regulations; |
| • | submission to the FDA of an IND which must become effective before human clinical trials may commence; |
| • | completion of adequate and well-controlled human clinical trials in accordance with good clinical practices, or GCPs, to establish that the biological product is “safe, pure and potent”, which is analogous to the safety and efficacy approval standard for a chemical drug product for its intended use; |
| • | submission to the FDA of a BLA; |
| • | satisfactory completion of an FDA preapproval inspection of the manufacturing facility or facilities at which the product is produced to assess compliance with applicable current good manufacturing practices, or cGMPs and in the case of our T-cell product candidates, good tissue practices, or GTPs; and |
105
| • | FDA review of the BLA and issuance of a biologics license. |
Before conducting studies in humans, laboratory evaluation of product chemistry, toxicity and formulation as well as animal studies to assess the potential safety and efficacy of the biologic candidate must be conducted. Preclinical toxicology studies in animals must be conducted in compliance with FDA regulations. The results of the preclinical tests, together with manufacturing information and analytical data, are submitted to the FDA as part of an IND. Some preclinical testing may continue even after the IND is submitted. In addition to including the results of the preclinical testing, the IND will also include a protocol detailing, among other things, the objectives of the clinical trial, the parameters to be used in monitoring safety and the effectiveness criteria to be evaluated if the first phase or phases of the clinical trial lend themselves to an efficacy determination. The IND will automatically become effective 30 days after receipt by the FDA, unless the FDA within the 30-day time period places the IND on clinical hold because of safety concerns about the product candidate or the conduct of the trial described in the clinical protocol included in the IND. The IND sponsor and the FDA must resolve any outstanding concerns before clinical trials can proceed.
All clinical trials for new drugs and biologics must be conducted under the supervision of one or more qualified principal investigators in accordance with GCPs. They must be conducted under protocols detailing the objectives of the applicable phase of the trial, dosing procedures, research subject selection and exclusion criteria and the safety and effectiveness criteria to be evaluated. Each protocol must be submitted to the FDA as part of the IND, and progress reports detailing the status of the clinical trials must be submitted to the FDA annually. Sponsors must also report to the FDA, within certain timeframes, serious and unexpected adverse reactions, any clinically important increase in the rate of a serious suspected adverse reaction over that listed in the protocol or investigator’s brochure, or any findings from other studies or animal or in vitro testing that suggest a significant risk in humans exposed to the product candidate. An institutional review board, or IRB, at each institution participating in the clinical trial must review and approve the protocol before a clinical trial commences at that institution, approve the information regarding the trial and the consent form that must be provided to each research subject or the subject’s legal representative, and monitor the trial until completed.
Clinical trials are typically conducted in three sequential phases, but the phases may overlap and different trials may be initiated with the same product candidate within the same phase of development in similar or differing patient populations. Phase 1 clinical studies may be conducted in a limited number of patients or healthy volunteers, as appropriate. The product candidate is initially tested for safety and, as appropriate, for absorption, metabolism, distribution, excretion, pharmacodynamics and pharmacokinetics.
Phase 2 usually involves trials in a larger, but still limited, patient population to evaluate preliminarily the efficacy of the product candidate for specific, targeted indications to determine dosage tolerance and optimal dosage and to identify possible short-term adverse effects and safety risks.
Phase 3 trials are undertaken to further evaluate clinical efficacy of a specific endpoint and to test further for safety within an expanded patient population at geographically dispersed clinical trial sites. Phase 1, Phase 2 or Phase 3 testing might not be completed successfully within any specific time period, if at all, with respect to any of our product candidates. Results from one trial are not necessarily predictive of results from later trials. Furthermore, the FDA or the sponsor may suspend clinical trials at any time on various grounds, including a finding that the subjects or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the product candidate has been associated with unexpected serious harm to patients.
106
The results of the preclinical studies and clinical trials, together with other detailed information, including information on the manufacture and composition of the product, are submitted to the FDA as part of a BLA requesting approval to market the product candidate for a proposed indication. Under the Prescription Drug User Fee Act the fees payable to the FDA for reviewing a BLA, as well as annual fees for commercial manufacturing establishments and for approved products, can be substantial but are subject to certain limited deferrals, waivers and reductions that may be available. The fees typically increase each year. Each BLA submitted to the FDA for approval is reviewed for administrative completeness and reviewability within 60 days following receipt by the FDA of the application. If the BLA is found complete, the FDA will file the BLA, triggering a full review of the application. The FDA may refuse to file any BLA that it deems incomplete or not properly reviewable at the time of submission. The FDA’s established goal is to review 90% of priority BLA applications within six months after the application is accepted for filing and 90% of standard BLA applications within 10 months of the acceptance date, whereupon a review decision is to be made. The FDA, however, may not approve a product candidate within these established goals and its review goals are subject to change from time to time. Further, the outcome of the review, even if generally favorable, may not be an actual approval but a “complete response letter” that describes additional work that must be done before the application can be approved. Before approving a BLA, the FDA may inspect the facility or facilities at which the product is manufactured and will not approve the product unless the facility complies with cGMPs. The FDA may deny approval of a BLA if applicable statutory or regulatory criteria are not satisfied, or may require additional testing or information, which can extend the review process. FDA approval of any application may include many delays or never be granted. If a product is approved, the approval may impose limitations on the uses for which the product may be marketed, may require that warning statements be included in the product labeling, may require that additional studies be conducted following approval as a condition of the approval, and may impose restrictions and conditions on product distribution, prescribing, or dispensing in the form of a Risk Evaluation and Mitigation Strategy, or REMS, or otherwise limit the scope of any approval. The FDA must approve a BLA supplement or a new BLA before a product may be marketed for other uses or before certain manufacturing or other changes may be made. Further post-marketing testing and surveillance to monitor the safety or efficacy of a product is required. Also, product approvals may be withdrawn if compliance with regulatory standards is not maintained or if safety or manufacturing problems occur following initial marketing. In addition, new government requirements may be established that could delay or prevent regulatory approval of our product candidates under development.
Under the Biologics Price Competition and Innovation Act of 2009, or the BPCIA, a statutory pathway has been created for licensure, or approval, of biological products that are biosimilar to, and possibly interchangeable with, earlier biological products licensed under the Public Health Service Act. Also under the BPCIA, innovator manufacturers of original reference biological products are granted 12 years of exclusivity before biosimilars can be approved for marketing in the United States. The implementation of an abbreviated approval pathway for biological products is under the direction of the FDA and is currently being developed. The FDA has issued several draft guidances for industry related to the BPCIA, addressing scientific, quality and procedural issues relevant to an abbreviated application for a biosimilar product. The approval of a biologic product biosimilar to one of our products could have a material adverse impact on our business as it may be significantly less costly to bring to market and may be priced significantly lower than our products.
Both before and after the FDA approves a product, the manufacturer and the holder or holders of the BLA for the product are subject to comprehensive regulatory oversight. For example, quality control and manufacturing procedures must conform, on an ongoing basis, to cGMP and GTP requirements, as applicable and the FDA periodically inspects manufacturing facilities to assess compliance with these standards. Accordingly, manufacturers must continue to spend time, money and effort to maintain compliance.
107
Orphan Drug Act
The Orphan Drug Act provides incentives to manufacturers to develop and market drugs for rare diseases and conditions affecting fewer than 200,000 persons in the United States at the time of application for orphan drug designation. Orphan drug designation must be requested before submitting a BLA. Orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process. If a product that has orphan drug designation subsequently receives the first FDA approval for the disease for which it has such designation, the holder of the approval is entitled to a seven-year exclusive marketing period in the United States for that product except in very limited circumstances. For example, a drug that the FDA considers to be clinically superior to, or different from, another approved orphan drug, even though for the same indication, may also obtain approval in the United States during the seven-year exclusive marketing period. In addition, holders of exclusivity for orphan drugs are expected to assure the availability of sufficient quantities of their orphan drugs to meet the needs of patients. Failure to do so could result in the withdrawal of marketing exclusivity for the drug.
Activin A has been strongly implicated in two subcategories of ovarian tumors: clear cell tumors and granulosa cell tumors. In these subcategories, we believe that we may be able to obtain orphan drug designation for STM 434 in the United States and, if supported by our clinical data, Breakthrough Therapy designation, and pursue clinical trials of STM 434 as a monotherapy. We believe that we may be able to obtain orphan drug designation in the United States for EBV-CTL in rituximab-refractory EBV-LPD after HCT and CMV-CTL in refractory CMV viremia and disease after HCT.
Legislation similar to the Orphan Drug Act has been enacted outside the United States, including in the EU. The orphan legislation in the EU is available for therapies addressing chronic debilitating or life-threatening conditions that affect five or fewer out of 10,000 persons or are financially not viable to develop. The market exclusivity period is for ten years, although that period can be reduced to six years if, at the end of the fifth year, available evidence establishes that the product is sufficiently profitable not to justify maintenance of market exclusivity. The market exclusivity may be extended to 12 years if sponsors complete a pediatric investigation plan agreed upon with the relevant committee of the EMA.
Expedited Review and Approval
The FDA has various programs, including Fast Track, priority review and accelerated approval, which are intended to expedite or simplify the process for developing and reviewing promising drugs, or to provide for the approval of a drug on the basis of a surrogate endpoint. Even if a drug qualifies for one or more of these programs, the FDA may later decide that the drug no longer meets the conditions for qualification or that the time period for FDA review or approval will be shortened. Generally, drugs that are eligible for these programs are those for serious or life-threatening conditions, those with the potential to address unmet medical needs and those that offer meaningful benefits over existing treatments. For example, Fast Track is a process designed to facilitate the development and expedite the review of drugs to treat serious or life-threatening diseases or conditions and fill unmet medical needs. Priority review is designed to give drugs that offer major advances in treatment or provide a treatment where no adequate therapy exists an initial review within six months as compared to a standard review time of 10 months. Although Fast Track and priority review do not affect the standards for approval, the FDA will attempt to facilitate early and frequent meetings with a sponsor of a Fast Track designated drug and expedite review of the application for a drug designated for priority review. Accelerated approval provides for an earlier approval for a new drug that is intended to treat a serious or life-threatening disease or condition and that fills an unmet medical need based on a surrogate endpoint. A surrogate endpoint is a laboratory measurement or physical sign used as an indirect or substitute measurement representing a clinically meaningful outcome. As a condition of approval, the
108
FDA may require that a sponsor of a product candidate receiving accelerated approval perform post-marketing clinical trials to confirm the clinically meaningful outcome as predicted by the surrogate marker trial.
In June 2013, the FDA published a draft Guidance for Industry titled, “Expedited Programs for Serious Conditions—Drugs and Biologics” which provides guidance on FDA programs that are intended to facilitate and expedite development and review of new drugs as well as threshold criteria generally applicable to concluding that a drug is a candidate for these expedited development and review programs. In addition to the Fast Track, accelerated approval and priority review programs discussed above, the FDA also provided guidance on Breakthrough Therapy designation. A request for Breakthrough Therapy designation should be submitted concurrently with, or as an amendment to an IND. FDA has already granted this designation to over 30 new drugs and has recently approved the first Breakthrough Therapy designated drugs.
Reimbursement
In both domestic and foreign markets, sales and reimbursement of any approved products will depend, in part, on the extent to which the costs of such products will be covered by third-party payors, such as government health programs, commercial insurance and managed healthcare organizations. These third-party payors are increasingly challenging the prices charged for medical products and services and imposing controls to manage costs. The containment of healthcare costs has become a priority of federal and state governments and the prices of drugs have been a focus in this effort. Governments have shown significant interest in implementing cost-containment programs, including price controls, restrictions on reimbursement and requirements for substitution of generic products. Adoption of price controls and cost-containment measures, and adoption of more restrictive policies in jurisdictions with existing controls and measures, could further limit our net revenue and results. In addition, there is significant uncertainty regarding the reimbursement status of newly approved healthcare products. We may need to conduct expensive pharmacoeconomic studies in order to demonstrate the cost-effectiveness of our products. If third-party payors do not consider our products to be cost-effective compared to other therapies, the payors may not cover our products after approved as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow us to sell our products on a profitable basis.
Within the United States, if we obtain appropriate approval in the future to market any of our current product candidates, we may seek approval and coverage for those products under Medicaid, Medicare and the Public Health Service, or PHS, pharmaceutical pricing program and also seek to sell the products to federal agencies.
Medicaid is a joint federal and state program that is administered by the states for low income and disabled beneficiaries. Under the Medicaid Drug Rebate Program, manufacturers are required to pay a rebate for each unit of product reimbursed by the state Medicaid programs. The amount of the rebate for each product is set by law and may be subject to an additional discount if certain pricing increases more than inflation.
Medicare is a federal program administered by the federal government that covers individuals age 65 and over as well as those with certain disabilities. Medicare Part D provides coverage to enrolled Medicare patients for self-administered drugs (i.e., drugs that do not need to be administered by a physician). Medicare Part D is administered by private prescription drug plans approved by the US government and each drug plan establishes its own Medicare Part D formulary for prescription drug coverage and pricing, which the drug plan may modify from time-to-time.
109
Medicare Part B covers most injectable drugs given in an in-patient setting, and some drugs administered by a licensed medical provider in hospital outpatient departments and doctors’ offices. Medicare Part B is administered by Medicare Administrative Contractors, which generally have the responsibility of making coverage decisions. Subject to certain payment adjustments and limits, Medicare generally pays for Part B covered drugs based on a percentage of manufacturer-reported average sales price.
Drug products are subject to discounted pricing when purchased by federal agencies via the Federal Supply Schedule, or FSS.
FFS participation is required for a drug product to be covered and paid for by certain federal agencies and for coverage under Medicaid, Medicare Part B and the PHS pharmaceutical pricing program. FSS pricing is negotiated periodically with the Department of Veterans Affairs. FSS pricing is intended to not exceed the price that a manufacturer charges its most-favored non-federal customer for its product. In addition, prices for drugs purchased by the Veterans Administration, Department of Defense (including drugs purchased by military personnel and dependents through the TRICARE retail pharmacy program), Coast Guard, and PHS are subject to a cap on pricing (known as the “federal ceiling price”) and may be subject to an additional discount if pricing increases more than inflation.
To maintain coverage of drugs under the Medicaid Drug Rebate Program, manufacturers are required to extend discounts to certain purchasers under the PHS pharmaceutical pricing program. Purchasers eligible for discounts include hospitals that serve a disproportionate share of financially needy patients, community health clinics and other entities that receive health services grants from the PHS.
The American Recovery and Reinvestment Act of 2009 provides funding for the federal government to compare the effectiveness of different treatments for the same illness. A plan for the research will be developed by the Department of Health and Human Services, the Agency for Healthcare Research and Quality and the National Institutes for Health, and periodic reports on the status of the research and related expenditures will be made to Congress. Although the results of the comparative effectiveness studies are not intended to mandate coverage policies for public or private payors, it is not clear what effect, if any, the research will have on the sales of any product, if any such product or the condition that it is intended to treat is the subject of a study. It is also possible that comparative effectiveness research demonstrating benefits in a competitor’s product could adversely affect the sales of any of our product candidates, if approved. If third-party payors do not consider our products to be cost-effective compared to other available therapies, they may not cover our products as a benefit under their plans or, if they do, the level of payment may not be sufficient to allow us to sell our products on a profitable basis.
The United States and state governments continue to propose and pass legislation designed to reduce the cost of healthcare. In March 2010, the United States Congress enacted the Patient Protection and Affordable Care Act and the Health Care and Education Reconciliation Act, or the Affordable Care Act, which included changes to the coverage and payment for drug products under government health care programs. Adoption of other new legislation at the federal or state level could further limit reimbursement for pharmaceuticals. Outside the United States, ensuring adequate coverage and payment for our products will face challenges. Pricing of prescription pharmaceuticals is subject to governmental control in many countries. Pricing negotiations with governmental authorities can extend well beyond the receipt of regulatory approval for a product and may require us to conduct a clinical trial that compares the cost effectiveness of our product candidates or products to other available therapies. The conduct of such a clinical trial could be expensive and result in delays in our commercialization efforts. Third-party payors are challenging the prices charged for medical products and services, and many third-party payors limit reimbursement for newly-approved health care
110
products. Recent budgetary pressures in many European Union countries are also causing governments to consider or implement various cost-containment measures, such as price freezes, increased price cuts and rebates. If budget pressures continue, governments may implement additional cost-containment measures. Cost-control initiatives could decrease the price we might establish for products that we may develop or sell, which would result in lower product revenues or royalties payable to us. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products.
Foreign Regulation
In addition to regulations in the United States, we expect to be subject to a variety of foreign regulations governing clinical trials and commercial sales and distribution of our product candidates. Whether or not we obtain FDA approval for a product candidate, we must obtain approval from the comparable regulatory authorities of foreign countries or economic areas, such as the European Union, before we may commence clinical trials or market products in those countries or areas. The approval process and requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary greatly from place to place, and the time may be longer or shorter than that required for FDA approval.
Certain countries outside of the United States have a process that requires the submission of a clinical trial application much like an IND prior to the commencement of human clinical trials. In Europe, for example, a clinical trial application, or CTA, must be submitted to the competent national health authority and to independent ethics committees in each country in which a company intends to conduct clinical trials. Once the CTA is approved in accordance with a country’s requirements, clinical trial development may proceed in that country. In all cases, the clinical trials must be conducted in accordance with GCPs and other applicable regulatory requirements.
Under European Union regulatory systems, a company may submit marketing authorization applications either under a centralized or decentralized procedure. The centralized procedure is compulsory for medicinal products produced by biotechnology or those medicinal products containing new active substances for specific indications such as the treatment of AIDS, cancer, neurodegenerative disorders, diabetes, viral diseases and designated orphan medicines, and optional for other medicines which are highly innovative. Under the centralized procedure, a marketing application is submitted to the European Medicines Agency where it will be evaluated by the Committee for Medicinal Products for Human Use and a favorable opinion typically results in the grant by the European Commission of a single marketing authorization that is valid for all European Union member states within 67 days of receipt of the opinion. The initial marketing authorization is valid for five years, but once renewed is usually valid for an unlimited period.
As in the United States, we may apply for designation of a product as an orphan drug for the treatment of a specific indication in the European Union before the application for marketing authorization is made. Orphan drugs in Europe enjoy economic and marketing benefits, including up to 11 years of exclusivity for the approved indication unless another applicant can show that its product is safer, more effective or otherwise clinically superior to the orphan designated product.
Additional Regulation
We are also subject to regulation under the Occupational Safety and Health Act, the Environmental Protection Act, the Toxic Substances Control Act, the Resource Conservation and Recovery Act and other present and potential federal, state or local regulations. These and other laws govern our use, handling and disposal of various biological and chemical substances used in, and
111
waste generated by our operations. Our research and development involves the controlled use of hazardous materials, chemicals and viruses. Although we believe that our safety procedures for handling and disposing of such materials comply with the standards prescribed by state and federal regulations, the risk of accidental contamination or injury from these materials cannot be completely eliminated. In the event of such an accident, we could be held liable for any damages that result and any such liability could exceed our resources.
There have been a number of federal and state proposals during the last few years regarding the pricing of pharmaceutical and biological products, government control and other changes to the healthcare system of the United States. It is uncertain what legislative proposals will be adopted or what actions federal, state or private payers for medical goods and services may take in response to any healthcare reform proposals or legislation. We cannot predict the effect medical or healthcare reforms may have on our business, and no assurance can be given that any such reforms will not have a material adverse effect.
Manufacturing
Our initial strategy is to outsource the manufacturing of drug substance and drug product for our preclinical studies and clinical trials. We also outsource fill-finish, packaging, labeling, storage, shipping and distribution. This allows us to rapidly conduct manufacturing activities for multiple programs in parallel. It also allows us to balance the requirements of multiple programs and avoid costly investment in manufacturing infrastructure and personnel before clinical data are available. Our internal capabilities and experience in the manufacturing of protein therapeutics encompass a broad range of activities including cell line development, process development, analytical development, formulation development, clinical and commercial scale GMP manufacturing, quality control and quality assurance. We have less substantial internal technical expertise in the manufacture of cellular therapeutics; however, we are currently building those capabilities through our ongoing hiring activities. This breadth of experience allows us to effectively oversee and direct the activities of our contract manufacturers and testing facilities. In selecting contract manufacturing organizations, or CMOs, to manufacture our product candidates, we generally strive to select the CMO based on the particular technical needs of the product candidate. In addition, we aim to work with CMOs that possess the requisite scale, expertise and experience to support clinical as well as commercial product manufacturing. Although this approach, when coupled with the range of CMO capabilities, requires us to utilize multiple CMOs in the manufacturing of our product candidates, we believe it may also mitigate the need for costly and time consuming process transfers later in development. Ultimately, we believe that our outsourced model and approach to CMO management will allow us to efficiently scale our manufacturing processes to support our current clinical development programs and the potential commercialization of our product candidates. As our product candidates progress towards potential marketing approvals, we may choose to build or acquire through other means our own manufacturing facilities in order to maintain more substantial control over our supply chain.
Our lead molecularly targeted product candidates, PINTA 745 and STM 434, are manufactured using readily available raw materials and established manufacturing procedures. PINTA 745 is a peptibody that is expressed by a recombinant strain of E. Coli. STM 434 is produced in bioreactors using hamster ovary cells that have been genetically engineered to produce this specific product candidate. All of our other molecularly targeted product candidates will also be produced in bioreactors using mammalian cells; however, other than ATA 842, we have yet to establish master cell banks and manufacturing procedures to support the production of these proteins.
Concurrent with the license of our existing molecularly targeted product candidates from Amgen, we acquired certain manufacturing process know-how related to producing clinical research-related drug supply. In the case of PINTA 745 and STM 434, this included GMP materials to support the
112
manufacturing of clinical trial material. In the case of our earlier stage molecularly targeted product candidates, this know-how was more limited in scope, as these product candidates were pre-master cell bank in stage of development at the time of licensing.
Our T-cell product candidates are currently manufactured by MSK using readily available raw materials and established manufacturing procedures. Both product candidates require blood from healthy, consenting third-party donors as starting materials. The manufacturing process involves co-culturing and incubating viral or cancer specific antigen transformed B-cells collected from the blood of third party-donors with T-cells collected from the same donor, all under GTPs. GTPs are FDA regulations and guidance documents that govern the methods used in, and the facilities and controls used for, the manufacture of human cells, tissues and cellular and tissue based products, or HCT/Ps, which are human cells or tissue intended for implantation, transplant, infusion or transfer into a human recipient. The primary intent of the GTP requirements is to ensure that cell and tissue based products are manufactured in a manner designed to prevent the introduction, transmission and spread of communicable disease. FDA regulations also require tissue establishments to register and list their HCT/Ps with the FDA and, when applicable, to evaluate donors through screening and testing.
Pursuant to our June 2015 license agreement with MSK, we acquired the right to use certain manufacturing process know-how related to producing clinical research-related drug supply. This included materials to support the manufacturing of clinical trial material including key starting materials and intermediates as well as existing inventory of clinical trial materials.
We and our CMOs will be required to make further investments in order to manufacture product for pivotal studies, as well as for commercialization, including potentially the construction or acquisition of a wholly-owned manufacturing facility. Over time, we will depend on manufacturing campaigns that will require the transfer of manufacturing processes to our CMOs. These may include modifications to the processes to suit the CMO’s facility and capability constraints, as well as product comparability testing. We have already transferred the downstream elements of the STM 434 manufacturing process, and we have initiated transfer of the upstream components of the STM 434 manufacturing process. We are also developing a refrigerated liquid formulation of the STM 434 drug product. We have also initiated process transfer activities for PINTA 745. We currently rely on MSK for the manufacture of our T-cell product candidates; however, we expect to transfer this process to a CMO prior to commercialization. As we progress further in clinical development to pivotal trials, we will also need to develop commercial-scale manufacturing processes for each product candidate consistent with the proposed dose and schedule to be used in clinical practice and at a cost sufficient to support profitable commercialization.
Employees
As of May 31, 2015, we had 29 full-time employees. All of our personnel are co-employees of Atara and TriNet, a professional human resource service organization. Under our agreement with TriNet, TriNet is a co-employer of our personnel, and is responsible for administering all payroll functions, including tax withholding, and providing health insurance and other benefits for these individuals. We reimburse TriNet for these costs and pay TriNet a fee for its services. We are responsible for, and control, all aspects of the hiring, retention, compensation, management and supervision of our personnel. We consider the terms of our contract with TriNet to be reasonable and customary and believe this arrangement provides substantial benefit to us, in the form of lower costs for employee benefits and reduced administrative burden on us.
113
CERTAIN RELATIONSHIPS AND RELATED PERSON TRANSACTIONS
The following is a description of transactions since our formation in August 2012, to which we have been a party, in which the amount involved exceeded or will exceed $120,000, and in which any of our executive officers, directors, promoters or holders of more than 5% of any class of our voting securities, or an affiliate or immediate family member thereof, had or will have a direct or indirect material interest, other than compensation, termination and change in control arrangements, which are described under “Executive Compensation” in our Definitive Proxy Statement for our 2015 annual meeting of stockholders. Dr. Ciechanover, our Chief Executive Officer and founder, and entities affiliated with Kleiner Perkins Caufield & Byers may be deemed to be promoters within the meaning of SEC rules under the Securities Act. We believe the terms obtained or consideration that we paid or received, as applicable, in connection with the transactions described below were comparable to terms available or the amounts that would be paid or received, as applicable, in arm’s-length transactions with unrelated third parties.
Series A Preferred Stock Financing
In October 2012, January 2013 and March 2013, we issued and sold an aggregate of 5,150,699 shares of our Series A preferred stock for approximately $3.90 per share, for aggregate consideration of approximately $20.1 million. The table below sets forth the number of shares of Series A preferred stock purchased by our executive officers, directors and stockholders who held more than 5% of any class of our voting securities and their affiliates, to the extent they purchased in excess of $120,000 of our Series A preferred stock. For each share of preferred stock set forth in the table below, the holder received one share of our common stock upon the closing of our initial public offering.
| Number of Shares of Series A Preferred Stock |
Aggregate Purchase Price |
|||||||
| Entities affiliated with Kleiner Perkins Caufield & Byers(1) |
1,282,050 | $ | 5,000,000 | |||||
| Entities affiliated with Domain Associates(2) |
1,282,050 | $ | 5,000,000 | |||||
| Entities affiliated with DAG Ventures |
1,282,050 | $ | 5,000,000 | |||||
| Inmobiliaria Carso S.A. de C.V. |
897,435 | $ | 3,500,000 | |||||
| Alexandria Real Estate Equities, Inc.(3) |
256,410 | $ | 1,000,000 | |||||
| (1) | Beth Seidenberg, a member of our board of directors, is affiliated with Kleiner Perkins Caufield & Byers. |
| (2) | Eckard Weber, a member of our board of directors, is associated with Domain Associates. Dr. Weber has no voting or dispositive control with respect to the shares held by entities affiliated with Domain Associates. |
| (3) | Joel S. Marcus, a member of our board of directors, is affiliated with Alexandria Real Estate Equities, Inc. |
Amgen Agreements and Series A-1 Preferred Stock Issuance
For a description of our agreements with Amgen, see “Business—License Agreements.” In consideration for entering into our exclusive license agreements with Amgen, we also issued 615,384 shares of our Series A-1 preferred stock to Amgen. Amgen received one share of our common stock for each share of Series A-1 preferred stock held by Amgen upon the closing of our initial public offering.
Series B Preferred Stock Financing
From November 2013 through January 2014, we issued and sold an aggregate of 6,532,432 shares of our Series B preferred stock for approximately $7.96 per share, for aggregate consideration
114
of approximately $52.0 million. The table below sets forth the number of shares of Series B preferred stock purchased by our executive officers, directors and stockholders who held more than 5% of any class of our voting securities and their affiliates, to the extent they purchased more than $120,000 of our Series B preferred stock. For each share of preferred stock set forth in the table below, the holder received one share of our common stock upon the closing of our initial public offering.
| Number of Shares of Series B Preferred Stock |
Aggregate Purchase Price |
|||||||
| Entities managed by The Baupost Group, L.L.C. |
1,695,913 | $ | 13,500,001 | |||||
| Celgene Corporation |
1,256,235 | $ | 10,000,000 | |||||
| Amgen Inc. |
628,117 | $ | 4,999,999 | |||||
| Entities affiliated with Domain Associates(1) |
625,382 | $ | 4,978,233 | |||||
| Entities affiliated with DAG Ventures |
625,382 | $ | 4,978,233 | |||||
| Entities affiliated with Kleiner Perkins Caufield & Byers(2) |
625,370 | $ | 4,978,129 | |||||
| Alexandria Real Estate Equities, Inc.(3) |
501,945 | $ | 3,995,631 | |||||
| Inmobiliaria Carso S.A. de C.V. |
437,767 | $ | 3,484,762 | |||||
| (1) | Eckard Weber, a member of our board of directors, is associated with Domain Associates. Dr. Weber has no voting or dispositive control with respect to the shares held by entities affiliated with Domain Associates. |
| (2) | Beth Seidenberg, a member of our board of directors, is affiliated with Kleiner Perkins Caufield & Byers. |
| (3) | Joel S. Marcus, a member of our board of directors, is affiliated with Alexandria Real Estate Equities, Inc. |
Voting Agreement
Prior to our initial public offering, we were party to a voting agreement with certain holders of our common stock and preferred stock, including certain of our named executive officers and directors and entities with which certain of our directors are affiliated, with respect to the election of our directors and certain other matters. The voting agreement terminated upon the closing of our initial public offering and none of our stockholders have any special rights regarding the election or designation of members of our board of directors.
Right of First Refusal and Co-Sale Agreement
Prior to our initial public offering, we were party to a right of first refusal and co-sale agreement with certain holders of our common stock and preferred stock, including certain of our named executive officers and directors and entities with which certain of our directors are affiliated. These rights of purchase and co-sale were terminated upon the closing of our initial public offering.
Investors’ Rights Agreement
We are party to an investors’ rights agreement with certain holders of our common stock issued upon conversion of our preferred stock, including certain of our named executive officers and directors and entities with which certain of our directors are affiliated. This agreement provides that such holders of common stock have the right to demand that we file a registration statement or request that their shares of common stock be covered by a registration statement that we are otherwise filing. With respect to this offering, the registration rights have been validly waived. In addition to the registration rights, the investors’ rights agreement provides for certain information rights and rights of first refusal. The provisions of the investors’ rights agreement, other than those relating to registration rights, terminated upon the closing of our initial public offering. For more information regarding this agreement, see “Description of Capital Stock—Registration Rights.”
115
Indemnification Agreements
We have entered into indemnity agreements with our directors and officers that provide, among other things, that we will indemnify such officer or director, under the circumstances and to the extent provided for therein, for all reasonable expenses and liabilities incurred with any action or proceeding brought against them by reason of the fact that they are serving in such capacity, and otherwise to the fullest extent permitted under Delaware law and our Bylaws.
MSK Option and License Agreements
In September 2014, we entered into an exclusive option agreement with MSK under which we acquired the right to exclusively license from MSK the worldwide rights to three clinical stage T-cell programs. The initial option period was for 12 months. In exchange for the exclusive option, we paid MSK $1.25 million in cash and issued 59,761 shares of our common stock to MSK. We and MSK have agreed to collaborate on further research to develop additional cellular therapies, which may include
T-cell programs targeted against other antigens and/or CAR-T, and which we also would hold an option to license, if developed.
In June 2015, we exercised the option and entered into a license agreement with MSK. Under the terms of the license agreement, MSK granted us a worldwide, exclusive license to under certain patent rights, know-how and a library of T-cells and cell lines, to research, develop, manufacture and commercialize T-cell products specific to CMV, EBV or WT1 that comprise or are based on or made using such licensed rights. MSK also agreed to transfer certain INDs related to the licensed products to us. We have agreed to use commercially reasonable efforts to commercialize the licensed products and, if commercialized, continue active marketing efforts for any commercialized licensed product through the term of the license agreement.
In connection with the option exercise and the execution of the license agreement, we will make an upfront cash payment to MSK of $4.5 million. We are obligated to make additional milestone payments of up to $33.0 million with respect to the three licensed clinical stage T-cell programs based on achievement of specified development, regulatory and sales-related milestones. We are also required to make escalating mid to high single-digit royalty payments based on sales of any licensed products. In addition, under certain circumstances, we must make certain minimum annual royalty payments to MSK, which are creditable against earned royalties owed for the same annual period. We are also obligated to pay a low double-digit percentage of consideration we receive for sublicensing the licensed rights.
The license agreement expires for each licensed T-cell product on a licensed product-by-licensed product basis and a country-by-country basis, on the latest of: (i) expiration of the last licensed patent rights related to such licensed product in such country, (ii) expiration of any market exclusivity period granted by law with respect to such licensed product in such country, and (iii) a specified number of years after the first commercial sale of the licensed product in such country. Upon expiration of the license agreement, the licenses granted to us will become non-exclusive royalty-free, perpetual and irrevocable. MSK may terminate the license agreement if we materially breach the agreement and do not cure such breach within a specified period or if we experience certain insolvency events.
116
Policies and Procedures for Transactions with Related Persons
We have adopted a policy that our executive officers, directors, nominees for election as a director, beneficial owners of more than 5% of any class of our common stock and any members of the immediate family of any of the foregoing persons are not permitted to enter into a related person transaction with us without the prior consent of our audit committee. Any request for us to enter into a transaction with an executive officer, director, nominee for election as a director, beneficial owner of more than 5% of any class of our voting securities or any member of the immediate family of any of the foregoing persons, in which the amount involved exceeds $120,000 and such person would have a direct or indirect interest, must first be presented to our audit committee for review, consideration and approval. In approving or rejecting any such proposal, our audit committee is to consider the material facts of the transaction, including, but not limited to, whether the transaction is on terms no less favorable than terms generally available to an unaffiliated third party under the same or similar circumstances and the extent of the related person’s interest in the transaction. All of the transactions described above were entered into prior to the adoption of such policy, but after presentation, consideration and approval by our board of directors.
117
The following table sets forth, as of May 31, 2015, information regarding beneficial ownership of our capital stock by:
| • | each person, or group of affiliated persons, known by us to beneficially own more than 5% of our common stock; |
| • | each of our named executive officers; |
| • | each of our directors; and |
| • | all of our current executive officers and directors as a group. |
Beneficial ownership is determined according to the rules of the SEC and generally means that a person has beneficial ownership of a security if he, she or it possesses sole or shared voting or investment power of that security, including RSUs pursuant to which securities may issue within 60 days of May 31, 2015. Except as indicated by the footnotes below, we believe, based on the information furnished to us, that the persons named in the table below have sole voting and investment power with respect to all shares of common stock shown that they beneficially own, subject to community property laws where applicable. The information does not necessarily indicate beneficial ownership for any other purpose, including for purposes of Sections 13(d) and 13(g) of the Securities Act.
Our calculation of the percentage of beneficial ownership prior to this offering is based on 24,525,822 shares of our common stock outstanding as of May 31, 2015. We have based our calculation of the percentage of beneficial ownership after this offering on shares of our common stock outstanding immediately after the closing of this offering, assuming no exercise of outstanding options and no exercise of the underwriters’ option to purchase up to additional shares of our common stock.
The table is based on information supplied by officers, directors and principal stockholders and Schedules 13D and 13G, if any, filed with the SEC.
118
Unless otherwise indicated, the address of each beneficial owner listed in the table below is c/o Atara Biotherapeutics, Inc., 701 Gateway Blvd., Suite 200, South San Francisco, California 94080.
| Name of beneficial owner |
Number of Shares Beneficially Owned |
Percentage of Shares Beneficially Owned |
||||||||||
| Before |
After |
|||||||||||
| 5% Stockholders: |
||||||||||||
| Entities affiliated with The Baupost Group, L.L.C(1) |
4,763,265 | 19.4 | % | % | ||||||||
| Entities managed by Kleiner Perkins Caufield & Byers(2) |
2,176,650 | 8.9 | % | % | ||||||||
| Entities affiliated with Domain Associates(3) |
1,957,432 | 8.0 | % | % | ||||||||
| Entities affiliated with DAG Ventures(4) |
1,907,432 | 7.8 | % | % | ||||||||
| Amgen Inc.(5) |
1,468,501 | 6.0 | % | % | ||||||||
| Entities affiliated with Fidelity Investments(6) |
1,348,015 | 5.5 | % | % | ||||||||
| Inmobiliaria Carso S.A. de C.V.(7) |
1,335,202 | 5.4 | % | % | ||||||||
| Celgene Corporation(8) |
1,256,235 | 5.1 | % | % | ||||||||
| Executive Officers and Directors: |
||||||||||||
| Isaac E. Ciechanover(9) |
1,120,930 | 4.6 | % | % | ||||||||
| Mitchall G. Clark(10) |
26,937 | * | * | |||||||||
| Christopher Haqq(11) |
287,081 | 1.2 | % | % | ||||||||
| John F. McGrath, Jr.(12) |
38,393 | * | * | |||||||||
| Gad Soffer.(13) |
66,829 | * | * | |||||||||
| Eric Dobmeier |
— | — | — | |||||||||
| Matthew K. Fust |
7,478 | * | * | |||||||||
| Carol Gallagher(14) |
62,656 | * | * | |||||||||
| Joel S. Marcus(15) |
912,355 | 3.7 | % | % | ||||||||
| Beth Seidenberg(2) |
2,176,650 | 8.9 | % | % | ||||||||
| Eckard Weber(3) |
— | — | — | |||||||||
| All executive officers and directors as a group (11 persons)(16) |
4,699,309 | 19.2 | % | % | ||||||||
| * | Represents beneficial ownership of less than 1% of the outstanding common stock. |
| (1) | The Baupost Group, L.L.C., or Baupost, is a registered investment adviser and acts as the investment adviser to certain private investment limited partnerships on whose behalf these securities were purchased, and in such capacity has voting and investment power with respect to such securities. None of the investment limited partnerships owns greater than 5% of any class of voting securities. SAK Corporation is the manager of Baupost, and Mr. Seth A. Klarman is the sole director of SAK Corporation. Mr. Klarman and SAK Corporation disclaim beneficial ownership of the securities. The principal business address for Baupost, SAK Corporation, Mr. Klarman and the investment limited partnerships is 10 St. James Avenue, Suite 1700, Boston, MA 02116. |
| (2) | Consists of 2,113,528 shares of common stock held by Kleiner Perkins Caufield & Byers XV, LLC, or KPCB XV, and 63,122 shares of common stock held by KPCB XV Founders Fund, LLC, or KPCB XV FF. All shares are held for convenience in the name of “KPCB Holdings, Inc., as nominee” for the accounts of such entities. The managing member of KPCB XV and KPCB XV FF is KPCB XV Associates, LLC, or KPCB XV Associates. Michael Abbott, L. John Doerr, William Gordon, Wen Hsieh, Randy Komisar, Matthew Murphy, Theodore Schlein and Dr. Seidenberg, the managing members of KPCB XV Associates, exercise shared voting and dispositive control over the shares held by KPCB XV. The principal business address for all entities and individuals affiliated with Kleiner Perkins Caufield & Byers is 2750 Sand Hill Road, Menlo Park, CA 94025. |
| (3) | Includes 1,941,542 shares of common stock held by Domain Partners VIII, L.P. and 15,890 shares of common stock held by DP VIII Associates, L.P. The general partner of Domain Partners VIII, L.P. and DP VIII Associates, L.P. is One Palmer Square Associates VIII, L.P. James C. Blair, Brian H. Dovey, Jesse I. Treu, Kathleen K. Schoemaker, Brian K. Halak and Nicole Vitullo, the managing members of One Palmer Square Associates VIII, L.L.C., share the power to vote or dispose of the shares held by each such entity. Dr. Weber, a member of our board of directors, is an employee of Domain Associates and a member of One Palmer Square Associates VIII, L.L.C. Dr. Weber has no voting or investment control with respect to any of the above-noted holdings. The principal business address of Domain Partners VIII, L.P. and DP VIII Associates, L.P. is One Palmer Square, Suite 515, Princeton, NJ 08542. |
| (4) | Includes 1,902,798 shares of common stock held by DAG Ventures V-QP, L.P. and 4,634 shares of common stock held by DAG Ventures V, L.P. The general partner of DAG Ventures V, L.P. is DAG Ventures Management V, LLC. John J. Cadeddu, Greg Williams, Young J. Chung, Nick Pianim and R. Thomas Goodrich, the managing members of DAG Ventures Management V, LLC, share the power to vote or dispose of the shares held by each such entity. The principal business address of DAG Ventures V-QP, L.P. and DAG Ventures V, L.P. is 251 Lytton Avenue, Suite 200, Palo Alto, CA 94301. |
119
| (5) | Includes 853,117 shares of common stock held by Amgen Investments Ltd., an affiliate of Amgen Inc., and 615,384 shares of common stock held by Amgen Inc. The address for Amgen Inc. is One Amgen Center Drive, Mail Stop 28-5-C, Thousand Oaks, CA 91320. |
| (6) | The address of FMR LLC, or FMR, is 245 Summer Street, Boston, Massachusetts 02210. FMR, along with certain of its subsidiaries and affiliates, and other companies, has the sole power to vote or direct the vote of 1,348,015 shares and the sole power to dispose or direct the disposition of 1,348,015 shares of common stock. Edward C. Johnson 3d is a Director and the Chairman of FMR LLC and Abigail P. Johnson is a Director, the Vice Chairman, the Chief Executive Officer and the President of FMR LLC. Members of the family of Edward C. Johnson 3d, including Abigail P. Johnson, are the predominant owners, directly or through trusts, of Series B voting common shares of FMR LLC, representing 49% of the voting power of FMR LLC. The Johnson family group and all other Series B shareholders have entered into a shareholders’ voting agreement under which all Series B voting common shares will be voted in accordance with the majority vote of Series B voting common shares. Accordingly, through their ownership of voting common shares and the execution of the shareholders’ voting agreement, members of the Johnson family may be deemed, under the Investment Company Act of 1940, to form a controlling group with respect to FMR LLC. Neither FMR LLC nor Edward C. Johnson 3d nor Abigail P. Johnson has the sole power to vote or direct the voting of the shares owned directly by the various investment companies registered under the Investment Company Act, or Fidelity Funds, advised by Fidelity Management & Research Company, or FMR Co, a wholly owned subsidiary of FMR LLC, which power resides with the Fidelity Funds’ Boards of Trustees. Fidelity Co carries out the voting of the shares under written guidelines established by the Fidelity Funds’ Boards of Trustees. This information is based solely upon a Schedule 13G filed by FMR LLC on February 13, 2015. |
| (7) | Represents shares held by Control Empresarial de Capitales, S.A. de C.V., a subsidiary of Inmobiliaria Carso S.A. de C.V., or Inmobiliaria. Carlos Slim Helú, Carlos Slim Domit, Marco Antonio Slim Domit, Patrick Slim Domit, María Soumaya Slim Domit, Vanessa Paola Slim Domit and Johanna Monique Slim Domit are beneficiaries of a Mexican trust that in turn owns substantially all of the issued and outstanding voting securities of Inmobiliaria. The address for this stockholder is c/o Inmobiliaria Carso S.A. de C.V., Paseo de las Palmas 750, 6th Floor, Lomas de Chapultepec, Mexico, D.F., 11000. |
| (8) | The address for this stockholder is 86 Morris Avenue, Summit, NJ 07901. |
| (9) | Represents 407,382 shares held by the Isaac E. Ciechanover and Allison M. Ciechanover Family Trust dated 8/8/08, 488,653 shares held by the Ciechanover Family GRAT, 180,000 shares held by the Ciechanover Family 2015 GRAT dated February 11, 2015 and 44,895 shares pursuant to options exercisable and RSUs expected to settle within 60 days of May 31, 2015. |
| (10) | Includes 18,959 shares held by Mr. Clark and 7,978 shares pursuant to options exercisable and RSUs expected to settle within 60 days of May 31, 2015. |
| (11) | Represents 252,540 shares held by Dr. Haqq, 20,000 shares held by Chris Haqq 2014 GRAT and 14,541 shares pursuant to options exercisable and RSUs expected to settle within 60 days of May 31, 2015. |
| (12) | Includes 25,727 shares held by Mr. McGrath and 12,666 shares pursuant to options exercisable and RSUs expected to settle within 60 days of May 31, 2015. |
| (13) | Includes 54,163 shares held by Mr. Soffer and 12,666 shares pursuant to options exercisable and RSUs expected to settle within 60 days of May 31, 2015. |
| (14) | Represents 62,656 shares held by the Gallagher Revocable Trust. |
| (15) | Represents 908,355 shares held by Alexandria Equities, LLC, an affiliate of Alexandria Real Estate Equities, Inc. and 4,000 shares held by the Joel S. Marcus and Barbara A. Marcus Family Trust. The address for this stockholder is 385 East Colorado Boulevard, Suite 299, Pasadena, CA 91101. |
| (16) | Includes 92,746 shares pursuant to options exercisable and RSUs expected to settle within 60 days of May 31, 2015. |
120
General
The following descriptions of our capital stock and certain provisions of our amended and restated certificate of incorporation and amended and restated bylaws are summaries and are qualified by reference to the amended and restated certificate of incorporation and the amended and restated bylaws. Copies of these documents are filed with the SEC as exhibits to our registration statement of which this prospectus forms a part.
Our amended and restated certificate of incorporation provides for common stock and authorizes shares of undesignated preferred stock, the rights, preferences and privileges of which may be designated from time to time by our board of directors.
Our authorized capital stock consists of 520,000,000 shares, all with a par value of $0.0001 per share, of which 500,000,000 shares are designated as common stock and 20,000,000 shares are designated as preferred stock.
As of May 31, 2015, we had outstanding 24,525,822 shares of common stock and no shares of preferred stock. Our outstanding capital stock was held by approximately 17 stockholders of record as of May 31, 2015. As of May 31, 2015, we also had outstanding RSUs for 621,132 shares of common stock and outstanding options to acquire 1,426,035 shares of common stock held by employees, directors and consultants pursuant to our 2012 and 2014 Plans.
Common Stock
The holders of our common stock are entitled to one vote per share on all matters submitted to a vote of our stockholders. Subject to preferences that may be applicable to any preferred stock outstanding at the time, the holders of outstanding shares of common stock are entitled to receive ratably any dividends declared by our board of directors out of assets legally available therefor. In the event that we liquidate, dissolve or wind up, holders of our common stock are entitled to share ratably in all assets remaining after payment of liabilities and the liquidation preference of any then outstanding shares of preferred stock. Holders of common stock have no preemptive or conversion rights or other subscription rights. There are no redemption or sinking fund provisions applicable to the common stock. All outstanding shares of common stock are, and all shares of common stock to be outstanding upon completion of this offering will be, fully paid and nonassessable.
Preferred Stock
Our board of directors may, without further action by our stockholders, fix the rights, preferences, privileges and restrictions of up to an aggregate of 20,000,000 shares of preferred stock in one or more series and authorize their issuance, subject to the approval rights of the common stock described above. These rights, preferences and privileges could include dividend rights, conversion rights, voting rights, terms of redemption, liquidation preferences, sinking fund terms and the number of shares constituting any series or the designation of such series, any or all of which may be greater than the rights of our common stock or common stock. The issuance of our preferred stock could adversely affect the voting power of holders of our common stock or common stock and the likelihood that such holders will receive dividend payments and payments upon liquidation. In addition, the issuance of preferred stock could have the effect of delaying, deferring or preventing a change of control or other corporate action. As of May 31, 2015, no shares of preferred stock were outstanding, and we have no present plan to issue any shares of preferred stock.
121
Registration Rights
We are party to an investors’ rights agreement that provides certain holders of our common stock, including certain holders of 5% of our capital stock and entities affiliated with certain of our directors, certain registration rights, as set forth below. The registration of shares of our common stock pursuant to the exercise of registration rights described below would enable the holders to sell these shares without restriction under the Securities Act when the applicable registration statement is declared effective. We will pay the registration expenses, other than the underwriting discounts and commissions, of the shares registered pursuant to the demand, piggyback and Form S-3 registrations described below.
Generally, in an underwritten offering, the managing underwriter, if any, has the right, subject to specified conditions, to limit the number of shares such holders may include. The demand, piggyback and Form S-3 registration rights described below will expire upon the earlier of October 16, 2019, which is five years following the consummation of our initial public offering, or with respect to an investor, when that investor, considered with its affiliates, can sell all of its shares in a three-month period under Rule 144.
Demand Registration Rights
The holders of certain shares of common stock outstanding as of May 31, 2015 are entitled to certain demand registration rights. The holders of at least 35% of these shares may, on not more than two occasions, request that we register all or a portion of their shares, subject to certain specified exceptions. Such request for registration must cover such number of shares such that the anticipated aggregate offering price would equal or exceed $30.0 million.
Piggyback Registration Rights
In connection with this offering, certain holders of shares of common stock were entitled to, and the necessary percentage of holders waived, their rights to notice of this offering and to include their shares of registrable securities in this offering. In the event that we propose to register any of our securities under the Securities Act in another offering, either for our own account or for the account of other security holders, the holders of these shares will be entitled to certain “piggyback” registration rights allowing them to include their shares in such registration, subject to certain marketing and other limitations. As a result, whenever we propose to file a registration statement under the Securities Act, including a registration statement on Form S-3 as discussed below, other than with respect to a demand registration or a registration statement on Forms S-4 or S-8 or related to stock issued upon conversion of debt securities, the holders of these shares are entitled to notice of the registration and have the right, subject to limitations that the underwriters may impose on the number of shares included in the registration, to include their shares in the registration.
Form S-3 Registration Rights
The holders of certain shares of common stock are entitled to certain Form S-3 registration rights. Any holder or holder of at least 25% of these shares can make a request that we register their shares on Form S-3 if we are qualified to file a registration statement on Form S-3, subject to certain specified exceptions. Such request for registration on Form S-3 must cover securities the aggregate offering price of which, before payment of the underwriting discounts and commissions, equals or exceeds $5.0 million. We will not be required to effect more than two registrations on Form S-3 within any 12-month period.
122
Anti-Takeover Provisions
Certificate of Incorporation and Bylaws
Because our stockholders do not have cumulative voting rights, our stockholders holding a majority of the outstanding shares of common stock outstanding will be able to elect all of our directors. Our amended and restated certificate of incorporation and amended and restated bylaws provide that all stockholder actions must be effected at a duly called meeting of stockholders and not by written consent. A special meeting of stockholders may be called by holders of a majority of our common stock and common stock, voting together as a single class, or by the majority of our whole board of directors, or our chief executive officer.
As described above in “Management—Board Composition,” in accordance with our amended and restated certificate of incorporation our board of directors is divided into three classes with staggered three-year terms.
The foregoing provisions will make it more difficult for our existing stockholders to replace our board of directors as well as for another party to obtain control of us by replacing our board of directors. Since our board of directors has the power to retain and discharge our officers, these provisions could also make it more difficult for existing stockholders or another party to effect a change in management. In addition, the authorization of undesignated preferred stock makes it possible for our board of directors to issue preferred stock with voting or other rights or preferences that could impede the success of any attempt to change our control.
These provisions are intended to enhance the likelihood of continued stability in the composition of our board of directors and its policies and to discourage certain types of transactions that may involve an actual or threatened acquisition of us. These provisions are also designed to reduce our vulnerability to an unsolicited acquisition proposal and to discourage certain tactics that may be used in proxy fights. However, such provisions could have the effect of discouraging others from making tender offers for our shares and may have the effect of deterring hostile takeovers or delaying changes in our control or management. As a consequence, these provisions also may inhibit fluctuations in the market price of our stock that could result from actual or rumored takeover attempts.
Section 203 of the Delaware General Corporation Law
We are subject to Section 203 of the Delaware General Corporation Law, which prohibits a Delaware corporation from engaging in any business combination with any interested stockholder for a period of three years after the date that such stockholder became an interested stockholder, with the following exceptions:
| • | before such date, the board of directors of the corporation approved either the business combination or the transaction that resulted in the stockholder becoming an interested stockholder; |
| • | upon closing of the transaction that resulted in the stockholder becoming an interested stockholder, the interested stockholder owned at least 85% of the voting stock of the corporation outstanding at the time the transaction began, excluding for purposes of determining the voting stock outstanding (but not the outstanding voting stock owned by the interested stockholder) those shares owned by (i) persons who are directors and also officers and (ii) employee stock plans in which employee participants do not have the right to determine confidentially whether shares held subject to the plan will be tendered in a tender or exchange offer; or |
| • | on or after such date, the business combination is approved by the board of directors and authorized at an annual or special meeting of the stockholders, and not by written consent, by the affirmative vote of at least 66 2/3% of the outstanding voting stock that is not owned by the interested stockholder. |
123
In general, Section 203 defines “business combination” to include the following:
| • | any merger or consolidation involving the corporation and the interested stockholder; |
| • | any sale, transfer, pledge or other disposition of 10% or more of the assets of the corporation involving the interested stockholder; |
| • | subject to certain exceptions, any transaction that results in the issuance or transfer by the corporation of any stock of the corporation to the interested stockholder; |
| • | any transaction involving the corporation that has the effect of increasing the proportionate share of the stock or any class or series of the corporation beneficially owned by the interested stockholder; or |
| • | the receipt by the interested stockholder of the benefit of any loss, advances, guarantees, pledges or other financial benefits by or through the corporation. |
In general, Section 203 defines an “interested stockholder” as an entity or person who, together with the person’s affiliates and associates, beneficially owns, or within three years prior to the time of determination of interested stockholder status did own, 15% or more of the outstanding voting stock of the corporation.
Choice of Forum
Our amended and restated certificate of incorporation provides that the Court of Chancery of the State of Delaware will be the exclusive forum for any derivative action or proceeding brought on our behalf; any action asserting a breach of fiduciary duty; any action asserting a claim against us arising pursuant to the Delaware General Corporation Law, our amended and restated certificate of incorporation or our bylaws; or any action asserting a claim against us that is governed by the internal affairs doctrine.
Limitations of Liability and Indemnification
Our amended and restated certificate of incorporation and restated bylaws provide that we will indemnify our directors and officers, and may indemnify our employees and other agents, to the fullest extent permitted by the Delaware General Corporation Law. However, Delaware law prohibits our amended and restated certificate of incorporation from limiting the liability of our directors for the following:
| • | any breach of a director’s duty of loyalty to us or to our stockholders; |
| • | acts or omissions not in good faith or that involve intentional misconduct or a knowing violation of law; |
| • | unlawful payment of dividends or unlawful stock repurchases or redemptions; and |
| • | any transaction from which a director derived an improper personal benefit. |
If Delaware law is amended to authorize corporate action further eliminating or limiting the personal liability of a director, then the liability of our directors will be eliminated or limited to the fullest extent permitted by Delaware law, as so amended. Our amended and restated certificate of incorporation does not eliminate a director’s duty of care and, in appropriate circumstances, equitable remedies, such as injunctive or other forms of non-monetary relief, remain available under Delaware law. It also does not affect a director’s responsibilities under any other laws, such as the federal securities laws or other state or federal laws. Under our amended and restated bylaws, we will also be empowered to enter into indemnification agreements with our directors, officers, employees and other agents and to purchase insurance on behalf of any person whom we are required or permitted to indemnify.
124
In addition to the indemnification required in our amended and restated certificate of incorporation and amended and restated bylaws, we have entered into indemnification agreements with each of our current directors and executive officers. These agreements provide for the indemnification of such persons for all reasonable expenses and liabilities incurred in connection with any action or proceeding brought against them by reason of the fact that they are or were serving in such capacity. We believe that these certificate of incorporation and bylaws provisions and indemnification agreements are necessary to attract and retain qualified persons as directors, officers and employees. Furthermore, we maintain director and officer liability insurance to cover liabilities our directors and officers may incur in connection with their services to us.
The limitation of liability and indemnification provisions in our amended and restated certificate of incorporation and amended and restated bylaws may discourage stockholders from bringing a lawsuit against directors for breach of their fiduciary duties. They may also reduce the likelihood of derivative litigation against directors and officers, even though an action, if successful, might benefit us and our stockholders. A stockholder’s investment may be harmed to the extent we pay the costs of settlement and damage awards against directors and officers pursuant to these indemnification provisions. Insofar as indemnification for liabilities arising under the Securities Act of 1933, as amended, or the Securities Act, may be permitted to our directors, officers and controlling persons pursuant to the foregoing provisions, or otherwise, we have been advised that, in the opinion of the SEC, such indemnification is against public policy as expressed in the Securities Act, and is, therefore, unenforceable. There is no pending litigation or proceeding naming any of our directors or officers as to which indemnification is being sought, nor are we aware of any pending or threatened litigation that may result in claims for indemnification by any director or officer.
Listing
Our common stock is listed on The Nasdaq Global Select Market under the symbol “ATRA.”
Transfer Agent and Registrar
The transfer agent and registrar for our common stock is Computershare Trust Company, N.A. The transfer agent and registrar’s address is 250 Royall Street, Canton, Massachusetts 02021.
125
SHARES ELIGIBLE FOR FUTURE SALE
Future sales of our common stock in the public market, or the availability of such shares for sale in the public market, could adversely affect market prices prevailing from time to time. As described below, only a limited number of shares will be available for sale shortly after this offering due to contractual and legal restrictions on resale. Nevertheless, sales of our common stock in the public market after such restrictions lapse, or the perception that those sales may occur, could adversely affect the prevailing market price at such time and our ability to raise equity capital in the future.
Based on the number of shares outstanding as of May 31, 2015, upon the closing of this offering, shares of common stock will be outstanding, assuming no exercise of the underwriters’ option to purchase additional shares of common stock, no exercise of outstanding options and no issuance of shares upon settlement of RSUs. Of the outstanding shares, all of the shares sold in this offering will be freely tradable, except that any shares held by our affiliates, as that term is defined in Rule 144 under the Securities Act, may only be sold in compliance with the limitations described below.
The remaining shares of our common stock outstanding after this offering are restricted securities as such term is defined in Rule 144 under the Securities Act and are subject to lock-up agreements with us as described below. Following the expiration of the applicable lock-up period, restricted securities may be sold in the public market only if registered or if they qualify for an exemption from registration under Rule 144 or 701 promulgated under the Securities Act, described in greater detail below.
Rule 144
In general, a person who has beneficially owned restricted shares of our common stock for at least six months would be entitled to sell their securities provided that (i) such person is not deemed to have been one of our affiliates at the time of, or at any time during the 90 days preceding, a sale and (ii) we are subject to the Exchange Act periodic reporting requirements for at least 90 days before the sale. Persons who have beneficially owned restricted shares of our common stock for at least six months but who are our affiliates at the time of, or any time during the 90 days preceding, a sale, would be subject to additional restrictions, by which such person would be entitled to sell within any three- month period only a number of securities that does not exceed the greater of either of the following:
| • | 1% of the number of shares of our common stock outstanding after this offering, which will equal shares based on the number of shares of common stock outstanding as of May 31, 2015 and assuming no exercise of the underwriters’ option to purchase additional shares of common stock; or |
| • | the average weekly trading volume of our common stock on The Nasdaq Global Select Market during the four calendar weeks preceding the filing of a notice on Form 144 with respect to the sale; |
provided in each case, that we are subject to the Exchange Act periodic reporting requirements for at least 90 days before the sale. Such sales both by affiliates and by non-affiliates must also comply with the manner of sale, current public information and notice provisions of Rule 144.
Rule 701
Rule 701 under the Securities Act, as in effect on the date of this prospectus, permits re-sales of shares in reliance upon Rule 144 but without compliance with certain restrictions of Rule 144, including the holding period requirement. Most of our employees, executive officers, directors or consultants who
126
purchased shares under a written compensatory plan or contract may be entitled to rely on the resale provisions of Rule 701, but all holders of Rule 701 shares are required to wait until 90 days after the date of this prospectus before selling their shares. However, substantially all Rule 701 shares are subject to lock-up agreements as described below and under “Underwriting” and will become eligible for sale at the expiration of those agreements.
Lock-Up Agreements
We and our executive officers and directors have agreed with the underwriters subject to certain exceptions, we and they will not, directly or indirectly, offer, sell, contract to sell, pledge, grant any option to purchase, make any short sale or otherwise dispose of or hedge any of our shares of common stock, any options or warrants to purchase shares of our common stock, or any securities convertible into, or exchangeable for or that represent the right to receive shares of our common stock for 90 days following the date of this prospectus. Funds managed by Kleiner Perkins Caufield & Byers and funds affiliated with Domain Associates have agreed with the underwriters, subject to certain exceptions, that they will not do any of the foregoing for 45 days following the date of this prospectus; provided, that after 30 days, the foregoing restrictions will not apply with respect to an aggregate of 600,000 of their shares. These lock-up agreements do not apply to an aggregate of up to shares that may be sold by our executive officers or directors pursuant to Rule 10b5-1 trading plans in place as of the date of this prospectus. Goldman, Sachs & Co. and Citigroup Global Markets, Inc. may, in their sole discretion, at any time, release all or any portion of the shares from the restrictions in such agreement.
Employees can only sell vested shares. Employees who do not hold vested shares, including shares subject to options, upon expiration of these selling restrictions will not be able to sell shares until they vest.
Registration Rights
The holders of certain shares of our common stock, or their transferees, are entitled to certain rights with respect to the registration of those shares under the Securities Act. For a description of these registration rights, see “Description of Capital Stock—Registration Rights.” If these shares are registered, they will be freely tradable without restriction under the Securities Act.
Equity Incentive Plans
We have filed a Form S-8 registration statement under the Securities Act to register shares of our common stock issued or reserved for issuance under our equity compensation plans and agreements. This registration statement became effective immediately upon filing, and shares covered by this registration statement are eligible for sale in the public markets, subject to vesting restrictions, the lock- up agreements described above and Rule 144 limitations applicable to affiliates. For a more complete discussion of our equity compensation plans, see “Executive Compensation—Employee Benefit Plans” in our Definitive Proxy Statement for our 2015 annual meeting of stockholders.
127
MATERIAL US FEDERAL INCOME TAX CONSEQUENCES TO
NON-US HOLDERS OF OUR COMMON STOCK
The following is a summary of the material US federal income tax consequences to non-US holders (as defined below) of the acquisition, ownership and disposition of our common stock issued pursuant to this offering. This discussion is not a complete analysis of all potential US federal income tax consequences relating thereto, does not address the potential application of the Medicare contribution tax and does not address any estate (except for the limited extent set forth below) or gift tax consequences or any tax consequences arising under any state, local or foreign tax laws, or any other US federal tax laws. This discussion is based on the Internal Revenue Code of 1986, as amended, or the Code, Treasury Regulations promulgated thereunder, judicial decisions and published rulings and administrative pronouncements of the Internal Revenue Service, or IRS, all as in effect as of the date of this prospectus. These authorities may change, possibly retroactively, resulting in US federal income tax consequences different from those discussed below. We have not requested a ruling from the U.S. Internal Revenue Service, or IRS, with respect to the statements made and the conclusions reached in the following summary, and there can be no assurance that the IRS will agree with such statements and conclusions.
This discussion is limited to non-US holders who purchase our common stock issued pursuant to this offering and who hold our common stock as a “capital asset” within the meaning of Section 1221 of the Code (generally, property held for investment). This discussion does not address all of the US federal income tax consequences that may be relevant to a particular holder in light of such holder’s particular circumstances. This discussion also does not consider any specific facts or circumstances that may be relevant to holders subject to special rules under the US federal income tax laws, including, without limitation, certain former citizens or long-term residents of the United States, partnerships or other pass-through entities, “controlled foreign corporations,” “passive foreign investment companies,” corporations that accumulate earnings to avoid US federal income tax, banks, financial institutions, investment funds, insurance companies, brokers, dealers or traders in securities, tax-exempt organizations, tax-qualified retirement plans, persons subject to the alternative minimum tax, persons that own, or have owned, actually or constructively, more than 5% of our common stock and persons holding our common stock as part of a hedging or conversion transaction or straddle, or a constructive sale, or other risk reduction strategy.
If an entity or arrangement that is classified as a partnership for US federal income tax purposes holds our common stock, the US federal income tax treatment of a partner will generally depend on the status of the partner and the activities of the partnership. Partnerships holding our common stock and the partners in such partnerships are urged to consult their tax advisors as to particular US federal income tax consequences to them of holding and disposing of our common stock.
PROSPECTIVE INVESTORS SHOULD CONSULT THEIR TAX ADVISORS REGARDING THE PARTICULAR US FEDERAL INCOME TAX CONSEQUENCES TO THEM OF ACQUIRING, OWNING AND DISPOSING OF OUR COMMON STOCK, AS WELL AS ANY TAX CONSEQUENCES ARISING UNDER ANY STATE, LOCAL OR FOREIGN TAX LAWS AND ANY OTHER US FEDERAL TAX LAWS.
Definition of Non-US Holder
For purposes of this discussion, a non-US holder is any beneficial owner of our common stock that is not a “US person” or a partnership (including any entity or arrangement treated as a partnership) for US federal income tax purposes. A US person is any of the following:
| • | an individual citizen or resident of the United States; |
128
| • | a corporation (or other entity treated as a corporation for US federal income tax purposes) created or organized under the laws of the United States, any state thereof or the District of Columbia; |
| • | an estate, the income of which is subject to US federal income tax regardless of its source; or |
| • | a trust (1) whose administration is subject to the primary supervision of a US court and which has one or more US persons who have the authority to control all substantial decisions of the trust, or (2) that has a valid election in effect under applicable Treasury Regulations to be treated as a US person. |
Distributions on Our Common Stock
If we make cash or other property distributions on our common stock, such distributions will constitute dividends for US federal income tax purposes to the extent paid from our current or accumulated earnings and profits, as determined under US federal income tax principles. Amounts not treated as dividends for US federal income tax purposes will constitute a return of capital and will first be applied against and reduce a holder’s tax basis in our common stock, but not below zero. Any excess will be treated as gain realized on the sale or other disposition of our common stock and will be treated as described under the section of this prospectus titled “—Gain on Disposition of our Common Stock” below.
Subject to the discussion below regarding backup withholding and FATCA, dividends (out of earnings and profits) paid to a non-US holder of our common stock generally will be subject to US federal withholding tax at a rate of 30% of the gross amount of the dividends, or such lower rate specified by an applicable income tax treaty. To receive the benefit of a reduced treaty rate, a non-US holder must furnish to us or our paying agent a valid IRS Form W-8BEN or IRS Form W-8BEN-E (or applicable successor form) including a US taxpayer identification number and certifying such holder’s qualification for the reduced rate. This certification must be provided to us or our paying agent prior to the payment of dividends and must be updated periodically. If the non-US holder holds the stock through a financial institution or other agent acting on the non-US holder’s behalf, the non-US holder will be required to provide appropriate documentation to the agent, which then will be required to provide certification to us or our paying agent, either directly or through other intermediaries.
Non-US holders that do not timely provide the required certification, but that qualify for a reduced treaty rate, may obtain a refund of any excess amounts withheld by timely filing an appropriate claim for refund with the IRS.
If a non-US holder holds our common stock in connection with the conduct of a trade or business in the United States, and dividends paid on our common stock are effectively connected with such holder’s US trade or business (and are attributable to such holder’s permanent establishment in the United States if required by an applicable tax treaty), the non-US holder will be exempt from US federal withholding tax. To claim the exemption, the non-US holder must generally furnish a properly executed IRS Form W-8ECI (or applicable successor form).
Any dividends paid on our common stock that are effectively connected with a non-US holder’s US trade or business (and if required by an applicable income tax treaty, are attributable to a permanent establishment maintained by the non-US holder in the United States) generally will be subject to US federal income tax on a net income basis at the regular graduated US federal income tax rates in the same manner as if such holder were a resident of the United States. A non-US holder that is a foreign corporation also may be subject to an additional branch profits tax equal to 30% (or such lower rate specified by an applicable income tax treaty) of its effectively connected earnings and profits
129
for the taxable year, as adjusted for certain items. Non-US holders should consult their tax advisors regarding any applicable income tax treaties that may provide for different rules.
Gain on Disposition of Our Common Stock
Subject to the discussion below regarding backup withholding and FATCA, a non-US holder generally will not be subject to US federal income tax on any gain realized upon the sale or other disposition of our common stock, unless:
| • | the gain is effectively connected with the non-US holder’s conduct of a trade or business in the United States, and if required by an applicable income tax treaty, is attributable to a permanent establishment maintained by the non-US holder in the United States; |
| • | the non-US holder is a nonresident alien individual present in the United States for 183 days or more during the taxable year of the disposition, and certain other requirements are met; or |
| • | our common stock constitutes a “United States real property interest” by reason of our status as a United States real property holding corporation, or USRPHC, for US federal income tax purposes at any time within the shorter of the five-year period preceding the disposition or the non-US holder’s holding period for our common stock, and our common stock is not regularly traded on an established securities market during the calendar year in which the sale or other disposition occurs. |
The determination of whether we are a USRPHC depends on the fair market value of our US real property interests relative to the fair market value of our other trade or business assets and our foreign real property interests. We believe we are not currently and do not anticipate becoming a USRPHC for US federal income tax purposes.
Gain described in the first bullet point above generally will be subject to US federal income tax on a net income basis at the regular graduated US federal income tax rates in the same manner as if such holder were a resident of the United States. A non-US holder that is a foreign corporation also may be subject to an additional branch profits tax equal to 30% (or such lower rate specified by an applicable income tax treaty) of its effectively connected earnings and profits for the taxable year, as adjusted for certain items. Non-US holders should consult their tax advisors regarding any applicable income tax treaties that may provide for different rules.Gain described in the second bullet point above will be subject to US federal income tax at a flat 30% rate (or such lower rate specified by an applicable income tax treaty), but may be offset by certain US-source capital losses (even though the individual is not considered a resident of the United States), provided that the non-US holder has timely filed US federal income tax returns with respect to such losses.
Information Reporting and Backup Withholding
Annual reports are required to be filed with the IRS and provided to each non-US holder indicating the amount of dividends on our common stock paid to such holder and the amount of any tax withheld with respect to those dividends. These information reporting requirements apply even if no withholding was required because the dividends were effectively connected with the holder’s conduct of a US trade or business, or withholding was reduced or eliminated by an applicable income tax treaty. This information also may be made available under a specific treaty or agreement with the tax authorities in the country in which the non-US holder resides or is established. Backup withholding, currently at a 28% rate, generally will not apply to payments to a non-US holder of dividends on or the gross proceeds of a disposition of our common stock provided the non-US holder furnishes the required certification as to its non-US status, such as by providing a valid IRS Form W-8BEN, IRS
130
Form W-8BEN-E or IRS Form W-8ECI, or certain other requirements are met. Notwithstanding the foregoing, backup withholding may apply if the payor has actual knowledge, or reason to know, that the holder is a US person who is not an exempt recipient.
Backup withholding is not an additional tax. If any amount is withheld under the backup withholding rules, the non-US holder should consult with a US tax advisor regarding the possibility of and procedure for obtaining a refund or a credit against the non-US holder’s US federal income tax liability, if any.
Withholding on Foreign Entities
Sections 1471 through 1474 of the Code (commonly referred to as FATCA) impose a US federal withholding tax of 30% on certain payments made to a “foreign financial institution” (as specially defined under these rules) unless such institution enters into an agreement with the US government to withhold on certain payments and to collect and provide to the US tax authorities substantial information regarding US account holders of such institution (which includes certain equity and debt holders of such institution, as well as certain account holders that are foreign entities with US owners) or an exemption applies. FATCA also generally will impose a US federal withholding tax of 30% on certain payments made to a non-financial foreign entity unless such entity provides the withholding agent a certification identifying the direct and indirect US owners of the entity or an exemption applies. An intergovernmental agreement between the United States and an applicable foreign country may modify these requirements. Under certain circumstances, a non-US holder might be eligible for refunds or credits of such taxes. FATCA currently will apply to dividends paid on our common stock. FATCA will also apply to gross proceeds from sales or other dispositions of our common stock after December 31, 2016.
Prospective investors are encouraged to consult with their own tax advisors regarding the possible implications of this legislation on their investment in our common stock.
Estate Tax
Individual non-US holders and entities whose property is potentially includible in such an individual’s gross estate for US federal estate tax purposes (for example, a trust funded by such an individual and with respect to which the individual has retained certain interests or powers), should note that, absent an applicable treaty benefit, our common stock generally will be treated as US situs property subject to US federal estate tax.
131
We and the underwriters named below have entered into an underwriting agreement with respect to the shares being offered. Subject to certain conditions, each underwriter has severally agreed to purchase the number of shares indicated in the following table. Goldman, Sachs & Co. and Citigroup Global Markets Inc. are the representatives of the underwriters.
| Underwriters |
Number of Shares | |
| Goldman, Sachs & Co. |
||
| Citigroup Global Markets Inc. |
||
| Canaccord Genuity Inc. |
||
| JMP Securities LLC |
||
| SunTrust Robinson Humphrey, Inc. |
||
|
| ||
| Total |
||
|
|
The underwriters are committed to take and pay for all of the shares being offered, if any are taken, other than the shares covered by the option described below unless and until this option is exercised.
The underwriters have an option to buy up to an additional shares of common stock from us. Any shares sold to the underwriters pursuant to the option will be sold at the public offering price, less underwriting discounts and commissions. They may exercise that option for 30 days. If any shares are purchased pursuant to this option, the underwriters will severally purchase shares in approximately the same proportion as set forth in the table above.
The following table shows the per share and total underwriting discounts and commissions to be paid to the underwriters. Such amounts are shown assuming both no exercise and full exercise of the underwriters’ option to purchase additional shares of common stock from us.
| Paid by Us |
No Exercise | Full Exercise | ||
| Per Share |
||||
|
|
| |||
| Total |
||||
|
|
|
Shares sold by the underwriters to the public will initially be offered at the public offering price set forth on the cover of this prospectus. Any shares sold by the underwriters to securities dealers may be sold at a discount of up to $ per share from the public offering price. After the initial offering of the shares, the representatives may change the offering price and the other selling terms. The offering of the shares by the underwriters is subject to receipt and acceptance and subject to the underwriters’ right to reject any order in whole or in part.
In connection with this offering, we and our executive officers and directors have agreed with the underwriters, subject to certain exceptions, not to dispose of or hedge any of our common stock or securities convertible into or exchangeable for shares of common stock for 90 days following the date of this prospectus, except with the prior written consent of the representatives. Funds managed by Kleiner Perkins Caufield & Byers and funds affiliated with Domain Associates have agreed with the underwriters, subject to certain exceptions, that they will not do any of the foregoing for 45 days following the date of this prospectus; provided, that after 30 days, the foregoing restrictions will not apply with respect to an aggregate of 600,000 of their shares. See “Shares Eligible for Future Sale” for a discussion of certain transfer restrictions.
Our common stock is listed on The Nasdaq Global Select Market under the symbol “ATRA.”
132
In connection with the offering, the underwriters may purchase and sell shares of our common stock in the open market. These transactions may include short sales, stabilizing transactions and purchases to cover positions created by short sales. Short sales involve the sale by the underwriters of a greater number of shares than they are required to purchase in the offering, and a short position represents the amount of such sales that have not been covered by subsequent purchases. A “covered short position” is a short position that is not greater than the amount of additional shares for which the underwriters’ option described above may be exercised. The underwriters may cover any covered short position by either exercising their option to purchase additional shares or purchasing shares in the open market. In determining the source of shares to cover the covered short position, the underwriters will consider, among other things, the price of shares available for purchase in the open market as compared to the price at which they may purchase additional shares pursuant to the option described above. “Naked” short sales are any short sales that create a short position greater than the amount of additional shares for which the option described above may be exercised. The underwriters must cover any such naked short position by purchasing shares in the open market. A naked short position is more likely to be created if the underwriters are concerned that there may be downward pressure on the price of our common stock in the open market after pricing that could adversely affect investors who purchase in the offering. Stabilizing transactions consist of various bids for or purchases of our common stock made by the underwriters in the open market prior to the completion of the offering.
The underwriters may also impose a penalty bid. This occurs when a particular underwriter repays to the underwriters a portion of the underwriting discount received by it because the representatives have repurchased shares sold by or for the account of such underwriter in stabilizing or short covering transactions.
Purchases to cover a short position and stabilizing transactions, as well as other purchases by the underwriters for their own accounts, may have the effect of preventing or retarding a decline in the market price of our stock, and together with the imposition of the penalty bid, may stabilize, maintain or otherwise affect the market price of our common stock. As a result, the price of the common stock may be higher than the price that otherwise might exist in the open market. The underwriters are not required to engage in these activities and may end any of these activities at any time. These transactions may be effected on The Nasdaq Global Select Market, in the over-the-counter market or otherwise.
The underwriters do not expect sales to discretionary accounts to exceed five percent of the total number of shares offered.
We estimate that our share of the total expenses of the offering, excluding underwriting discounts and commissions, will be approximately $ , including up to $ of expenses that we have agreed to reimburse the underwriters for costs relating to clearance of this offering with the Financial Industry Regulatory Authority, Inc.
We have agreed to indemnify the several underwriters against certain liabilities, including liabilities under the Securities Act.
The underwriters and their respective affiliates are full service financial institutions engaged in various activities, which may include sales and trading, commercial and investment banking, advisory, investment management, investment research, principal investment, hedging, market making, brokerage and other financial and non-financial activities and services. Certain of the underwriters and their respective affiliates have provided, and may in the future provide, a variety of these services to us and to persons and entities with relationships with us, for which they received or will receive customary fees and expenses.
133
In the ordinary course of their various business activities, the underwriters and their respective affiliates, officers, directors and employees may purchase, sell or hold a broad array of investments and actively trade securities, derivatives, loans, commodities, currencies, credit default swaps and other financial instruments for their own account and for the accounts of their customers, and such investment and trading activities may involve or relate to our assets, securities and/or instruments (directly, as collateral securing other obligations or otherwise) and/or persons and entities with relationships with us. The underwriters and their respective affiliates may also communicate independent investment recommendations, market color or trading ideas and/or publish or express independent research views in respect of such assets, securities or instruments and may at any time hold, or recommend to clients that they should acquire, long and/or short positions in such assets, securities and instruments.
European Economic Area
In relation to each Member State of the European Economic Area which has implemented the Prospectus Directive (each, a Relevant Member State), each underwriter has represented and agreed that with effect from and including the date on which the Prospectus Directive is implemented in that Relevant Member State (the Relevant Implementation Date) it has not made and will not make an offer of shares to the public in that Relevant Member State prior to the publication of a prospectus in relation to the shares which has been approved by the competent authority in that Relevant Member State or, where appropriate, approved in another Relevant Member State and notified to the competent authority in that Relevant Member State, all in accordance with the Prospectus Directive, except that it may, with effect from and including the Relevant Implementation Date, make an offer of shares to the public in that Relevant Member State at any time:
| (a) | to any legal entity which is a qualified investor as defined in the Prospectus Directive; |
| (b) | to fewer than 100 or, if the Relevant Member State has implemented the relevant provision of the 2010 PD Amending Directive, 150, natural or legal persons (other than qualified investors as defined in the Prospectus Directive), as permitted under the Prospectus Directive, subject to obtaining the prior consent of the representatives for any such offer; or |
| (c) | in any other circumstances falling within Article 3(2) of the Prospectus Directive, provided that no such offer of shares of our common stock shall result in a requirement for the publication by us or any underwriter of a prospectus pursuant to Article 3 of the Prospectus Directive. |
For the purposes of this provision, the expression an “offer of shares to the public” in relation to any shares in any Relevant Member State means the communication in any form and by any means of sufficient information on the terms of the offer and the shares to be offered so as to enable an investor to decide to purchase or subscribe for the shares, as the same may be varied in that Relevant Member State by any measure implementing the Prospectus Directive in that Relevant Member State and the expression Prospectus Directive means Directive 2003/71/EC (and amendments thereto, including the 2010 PD Amending Directive) and includes any relevant implementing measure in each Relevant Member State, and the expression “2010 PD Amending Directive” means Directive 2010/73/EU.
United Kingdom
Each underwriter has represented and agreed that:
| (a) | it has only communicated or caused to be communicated and will only communicate or cause to be communicated an invitation or inducement to engage in investment activity (within the meaning of Section 21 of the FSMA) received by it in connection with the issue or sale of the shares in circumstances in which Section 21(1) of the FSMA does not apply to the Issuer; and |
134
| (b) | it has complied and will comply with all applicable provisions of the FSMA with respect to anything done by it in relation to the shares in, from or otherwise involving the United Kingdom. |
France
Neither this prospectus nor any other offering material relating to the shares described in this prospectus has been submitted to the clearance procedures of the Autorité des Marchés Financiers or of the competent authority of another member state of the European Economic Area and notified to the Autorité des Marchés Financiers. The shares have not been offered or sold and will not be offered or sold, directly or indirectly, to the public in France. Neither this prospectus nor any other offering material relating to the shares has been or will be:
| • | released, issued, distributed or caused to be released, issued or distributed to the public in France; or |
| • | used in connection with any offer for subscription or sale of the shares to the public in France. |
Such offers, sales and distributions will be made in France only:
| • | to qualified investors (investisseurs qualifiés) and/or to a restricted circle of investors (cercle restreint d’investisseurs), in each case investing for their own account, all as defined in, and in accordance with articles L.411-2, D.411-1, D.411-2, D.734-1, D.744-1, D.754-1 and D.764-1 of the French Code monétaire et financier; |
| • | to investment services providers authorized to engage in portfolio management on behalf of third parties; or |
| • | in a transaction that, in accordance with article L.411-2-II-1°-or-2°-or 3° of the French Code monétaire et financier and article 211-2 of the General Regulations (Règlement Général) of the Autorité des Marchés Financiers, does not constitute a public offer (appel public à l’épargne). |
The shares may be resold directly or indirectly, only in compliance with articles L.411-1, L.411-2, L.412-1 and L.621-8 through L.621-8-3 of the French Code monétaire et financier.
Australia
No prospectus or other disclosure document (as defined in the Corporations Act 2001 (Cth) of Australia, or Corporations Act) in relation to the common stock has been or will be lodged with the Australian Securities & Investments Commission, or ASIC. This document has not been lodged with ASIC and is only directed to certain categories of exempt persons. Accordingly, if you receive this document in Australia:
| (a) | you confirm and warrant that you are either: |
| (i) | a “sophisticated investor” under section 708(8)(a) or (b) of the Corporations Act; |
| (ii) | a “sophisticated investor” under section 708(8)(c) or (d) of the Corporations Act and that you have provided an accountant’s certificate to us which complies with the requirements of section 708(8)(c)(i) or (ii) of the Corporations Act and related regulations before the offer has been made; |
| (iii) | a person associated with the company under section 708(12) of the Corporations Act; or |
135
| (iv) | a “professional investor” within the meaning of section 708(11)(a) or (b) of the Corporations Act, and to the extent that you are unable to confirm or warrant that you are an exempt sophisticated investor, associated person or professional investor under the Corporations Act any offer made to you under this document is void and incapable of acceptance; and |
| (b) | you warrant and agree that you will not offer any of the common stock for resale in Australia within 12 months of that common stock being issued unless any such resale offer is exempt from the requirement to issue a disclosure document under section 708 of the Corporations Act. |
Hong Kong
The shares may not be offered or sold by means of any document other than (i) in circumstances which do not constitute an offer to the public within the meaning of the Companies Ordinance (Cap.32, Laws of Hong Kong), (ii) to “professional investors” within the meaning of the Securities and Futures Ordinance (Cap.571, Laws of Hong Kong) and any rules made thereunder, or (iii) in other circumstances which do not result in the document being a “prospectus” within the meaning of the Companies Ordinance (Cap.32, Laws of Hong Kong), and no advertisement, invitation or document relating to the shares may be issued or may be in the possession of any person for the purpose of issue (in each case whether in Hong Kong or elsewhere), which is directed at, or the contents of which are likely to be accessed or read by, the public in Hong Kong (except if permitted to do so under the laws of Hong Kong) other than with respect to shares which are or are intended to be disposed of only to persons outside Hong Kong or only to “professional investors” within the meaning of the Securities and Futures Ordinance (Cap. 571, Laws of Hong Kong) and any rules made thereunder.
Singapore
This prospectus has not been registered as a prospectus with the Monetary Authority of Singapore. Accordingly, this prospectus and any other document or material in connection with the offer or sale, or invitation for subscription or purchase, of the shares may not be circulated or distributed, nor may the shares be offered or sold, or be made the subject of an invitation for subscription or purchase, whether directly or indirectly, to persons in Singapore other than (i) to an institutional investor under Section 274 of the Securities and Futures Act, Chapter 289 of Singapore, or the SFA, (ii) to a relevant person, or any person pursuant to Section 275(1A), and in accordance with the conditions, specified in Section 275 of the SFA or (iii) otherwise pursuant to, and in accordance with the conditions of, any other applicable provision of the SFA.
Where the shares are subscribed or purchased under Section 275 by a relevant person which is: (a) a corporation (which is not an accredited investor) the sole business of which is to hold investments and the entire share capital of which is owned by one or more individuals, each of whom is an accredited investor; or (b) a trust (where the trustee is not an accredited investor) whose sole purpose is to hold investments and each beneficiary is an accredited investor, shares, debentures and units of shares and debentures of that corporation or the beneficiaries’ rights and interest in that trust shall not be transferable for 6 months after that corporation or that trust has acquired the shares under Section 275 except: (1) to an institutional investor under Section 274 of the SFA or to a relevant person, or any person pursuant to Section 275(1A), and in accordance with the conditions, specified in Section 275 of the SFA; (2) where no consideration is given for the transfer; or (3) by operation of law.
136
Japan
The securities have not been and will not be registered under the Financial Instruments and Exchange Law of Japan (the Financial Instruments and Exchange Law) and each underwriter has agreed that it will not offer or sell any securities, directly or indirectly, in Japan or to, or for the benefit of, any resident of Japan (which term as used herein means any person resident in Japan, including any corporation or other entity organized under the laws of Japan), or to others for re-offering or resale, directly or indirectly, in Japan or to a resident of Japan, except pursuant to an exemption from the registration requirements of, and otherwise in compliance with, the Financial Instruments and Exchange Law and any other applicable laws, regulations and ministerial guidelines of Japan.
137
Cooley LLP of San Francisco, California is serving as our counsel in this offering. Davis Polk & Wardwell LLP of Menlo Park, California is representing the underwriters in this offering.
The financial statements incorporated in this prospectus by reference from our Annual Report on Form 10-K for the year ended December 31, 2014 have been audited by Deloitte & Touche LLP, an independent registered public accounting firm, as stated in their report, which is incorporated herein by reference. Such financial statements have been so incorporated in reliance upon the report of such firm given upon their authority as experts in accounting and auditing.
WHERE YOU CAN FIND MORE INFORMATION
We have filed with the SEC a registration statement on Form S-1 under the Securities Act with respect to this offering of our common stock. This prospectus, which constitutes a part of the registration statement, does not contain all of the information set forth in the registration statement, some items of which are contained in exhibits to the registration statement as permitted by the rules and regulations of the SEC. For further information with respect to us and our common stock, we refer you to the registration statement, including the exhibits and the financial statements and notes filed as a part of the registration statement. Statements contained in this prospectus concerning the contents of any contract or any other document are not necessarily complete. If a contract or document has been filed as an exhibit to the registration statement, please see the copy of the contract or document that has been filed. Each statement in this prospectus relating to a contract or document filed as an exhibit is qualified in all respects by the filed exhibit. The exhibits to the registration statement should be referenced for the complete contents of these contracts and documents. A copy of the registration statement and the exhibits filed therewith may be inspected without charge at the public reference room of the SEC, located at 100 F Street, N.E., Room 1580, Washington, D.C. 20549. You may obtain information on the operation of the public reference rooms by calling the SEC at 1-800-SEC-0330. The SEC also maintains an Internet website that contains reports, proxy statements and other information about issuers, like us, that file electronically with the SEC. The address of that website is www.sec.gov.
We are subject to the information and reporting requirements of the Exchange Act and, in accordance with this law, we file periodic reports, proxy statements and other information with the SEC. These periodic reports, proxy statements and other information is available for inspection and copying at the SEC’s public reference facilities and the website of the SEC referred to above. We also maintain a website at www.atarabio.com. You may access our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act with the SEC free of charge at our website as soon as reasonably practicable after such material is electronically filed with, or furnished to, the SEC. The information contained in, or that can be accessed through, our website is not part of this prospectus.
138
INCORPORATION OF CERTAIN INFORMATION BY REFERENCE
The SEC allows us to “incorporate by reference” information from other documents that we file with it, which means that we can disclose important information to you by referring you to those documents. The information incorporated by reference is considered to be part of this prospectus. Information in this prospectus supersedes information incorporated by reference that we filed with the SEC prior to the date of this prospectus. We incorporate by reference into this prospectus and the registration statement of which this prospectus is a part the information or documents listed below that we have filed with the SEC (SEC File No. 001-36548):
| • | our Annual Report on Form 10-K for the year ended December 31, 2014, filed with the SEC on February 26, 2015; |
| • | Amendment No. 1 to our Annual Report on Form 10-K for the year ended December 31, 2014, filed with the SEC on March 6, 2015; |
| • | the information specifically incorporated by reference into our Annual Report on Form 10-K for the year ended December 31, 2014 from our Definitive Proxy Statement on Schedule 14A, filed with the SEC on April 29, 2015; |
| • | our Quarterly Report on Form 10-Q for the quarter ended March 31, 2015, filed with the SEC on May 11, 2015; |
| • | our Current Reports on Form 8-K filed with the SEC on January 21, 2015, March 27, 2015, June 15, 2015 and June 29, 2015; and |
| • | the description of our common stock contained in our registration statement on Form 8-A filed with the SEC on July 16, 2014, including any amendments or reports filed for the purposes of updating this description. |
We will furnish without charge to you, on written or oral request, a copy of any or all of the documents incorporated by reference in this prospectus, including exhibits to these documents. You should direct any requests for documents to Investor Relations, Atara Biotherapeutics, Inc., 701 Gateway Boulevard, Suite 200, South San Francisco, CA 94080; telephone: (650) 278-8930.
You also may access these filings on our website at www.atarabio.com. We do not incorporate the information on our website into this prospectus or any supplement to this prospectus and you should not consider any information on, or that can be accessed through, our website as part of this prospectus or any supplement to this prospectus (other than those filings with the SEC that we specifically incorporate by reference into this prospectus or any supplement to this prospectus).
Any statement contained in a document incorporated or deemed to be incorporated by reference in this prospectus will be deemed modified, superseded or replaced for purposes of this prospectus to the extent that a statement contained in this prospectus modifies, supersedes or replaces such statement.
139
$125,000,000
Common Stock
| Goldman, Sachs & Co. | Citigroup |
| Canaccord Genuity | JMP Securities | SunTrust Robinson Humphrey | ||
PART II
Information Not Required in Prospectus
Item 13. Other Expenses of Issuance and Distribution
The following table sets forth the costs and expenses, other than the underwriting discounts and commissions, payable in connection with the sale and distribution of the securities being registered. All amounts are estimated except the SEC registration fee and the FINRA filing fee. Except as otherwise noted, all the expenses below will be paid by us.
| SEC registration fee |
$ | 16,704 | ||
| FINRA filing fee |
22,063 | |||
| Legal fees and expenses |
* | |||
| Accounting fees and expenses |
* | |||
| Printing and engraving expenses |
* | |||
| Transfer agent and registrar fees and expenses |
* | |||
| Miscellaneous fees and expenses |
* | |||
|
|
|
| ||
| Total |
$ * | |||
|
|
|
|
| * | To be completed by amendment. |
Item 14. Indemnification of Directors and Officers
Section 145 of the Delaware General Corporation Law authorizes a court to award, or a corporation’s board of directors to grant, indemnity to directors and officers in terms sufficiently broad to permit such indemnification under certain circumstances for liabilities, including reimbursement for expenses incurred, arising under the Securities Act of 1933, as amended. Our amended and restated certificate of incorporation provides for indemnification of our directors, officers, employees and other agents to the maximum extent permitted by the Delaware General Corporation Law, and our amended and restated bylaws provide for indemnification of our directors, officers, employees and other agents to the maximum extent permitted by the Delaware General Corporation Law.
We have entered into indemnification agreements with our directors and executive officers, whereby we have agreed to indemnify our directors and executive officers to the fullest extent permitted by law, including indemnification against expenses and liabilities incurred in legal proceedings to which the director or executive officer was, or is threatened to be made, a party by reason of the fact that such director or executive officer is or was our director, officer, employee or agent, provided that such director or executive officer acted in good faith and in a manner that the director or executive officer reasonably believed to be in, or not opposed to, the our best interest. At present, there is no pending litigation or proceeding involving any of our directors or executive officers regarding which indemnification is sought, nor are we aware of any threatened litigation that may result in claims for indemnification.
We maintain insurance policies that indemnify our directors and officers against various liabilities arising under the Securities Act of 1933, as amended, and the Securities Exchange Act of 1934, as amended, that might be incurred by any director or officer in his capacity as such.
The underwriters are obligated, under certain circumstances, pursuant to the underwriting agreement to be filed as Exhibit 1.1 hereto, to indemnify us, our officers and our directors against liabilities under the Securities Act of 1933, as amended.
II-1
Item 15. Recent Sales of Unregistered Securities
The following sets forth information regarding all unregistered securities sold since the inception of the registrant in August 2012 (share and per share amounts give effect to a 1.3-to-1 reverse split of our outstanding common stock and preferred that was effected on July 9, 2014):
| (a) | We issued 923,076 shares of common stock for a price of $0.0013 per share in August 2012 and March 2013 (which shares were contributed back to the capital of the company in connection with the recapitalization described in the prospectus forming part of this registration statement); |
| (b) | We issued 2,104,613 shares of common stock and 12,298,515 shares of preferred stock to the stockholders of Nina Biotherapeutics, Inc., Pinta Biotherapeutics, Inc. and Santa Maria Biotherapeutics, Inc. in such recapitalization, at a rate of one share of common stock or preferred stock of the company, respectively, for one share of common stock and preferred stock, respectively, of each of Nina Biotherapeutics, Inc., Pinta Biotherapeutics, Inc. and Santa Maria Biotherapeutics, Inc.; |
| (c) | We issued RSUs for 893,651 shares of common stock and options to purchase 554,969 shares of common stock to our employees, directors and consultants; and |
| (d) | We issued 59,761 shares of common stock to Memorial Sloan Kettering Cancer Center in connection with the execution of our exclusive option agreement in September 2014. |
The offers, sales and issuances of the securities described in Item 15(a) were deemed to be exempt from registration under the Securities Act under either (1) Rule 701 promulgated under the Securities Act as offers and sale of securities pursuant to certain compensatory benefit plans and contracts relating to compensation in compliance with Rule 701 or (2) Section 4(2) of the Securities Act as transactions by an issuer not involving any public offering. The recipients of securities in each of these transactions represented their intention to acquire the securities for investment only and not with view to or for sale in connection with any distribution thereof and appropriate legends were affixed to the stock certificates and instruments issued in such transactions.
Item 16. Exhibits and Financial Statement Schedules
(a) Exhibits.
The exhibits to the registration statement are listed in the Exhibit Index attached hereto and incorporated by reference herein.
(b) Financial statement schedules.
All schedules have been omitted because the information required to be presented in them is not applicable or is shown in the combined and consolidated financial statements or related notes.
Item 17. Undertakings
The undersigned Registrant hereby undertakes to provide to the underwriters at the closing specified in the Underwriting Agreement, certificates in such denominations and registered in such names as required by the underwriters to permit prompt delivery to each purchaser.
Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of the Registrant pursuant to the foregoing provisions, or otherwise, the Registrant has been advised that in the opinion of the Securities and Exchange Commission such indemnification is against public policy as expressed in the Securities Act and is,
II-2
therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by the Registrant of expenses incurred or paid by a director, officer or controlling person of the Registrant in the successful defense of any action, suit or proceeding) is asserted by such director, officer or controlling person in connection with the securities being registered, the Registrant will, unless in the opinion of its counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
The undersigned Registrant hereby undertakes that:
| (1) | For purposes of determining any liability under the Securities Act, the information omitted from the form of prospectus filed as part of this Registration Statement in reliance upon Rule 430A and contained in a form of prospectus filed by the Registrant pursuant to Rule 424(b)(1) or (4) or 497(h) under the Securities Act shall be deemed to be part of this Registration Statement as of the time it was declared effective. |
| (2) | For the purpose of determining any liability under the Securities Act, each post-effective amendment that contains a form of prospectus shall be deemed to be a new registration statement relating to the securities offered therein, and the offering of such securities at that time shall be deemed to be the initial bona fide offering thereof. |
II-3
SIGNATURES
Pursuant to the requirements of the Securities Act of 1933, we have duly caused this Registration Statement on Form S-1 to be signed on its behalf by the undersigned, thereunto duly authorized, in the City of South San Francisco, State of California, on the 29th day of June, 2015.
| ATARA BIOTHERAPEUTICS, INC. | ||
| By: |
/s/ Isaac E. Ciechanover | |
| Isaac E. Ciechanover Chief Executive Officer | ||
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Isaac E. Ciechanover and John F. McGrath, Jr., and each of them, as his or her true and lawful attorneys-in-fact and agents, each with the full power of substitution, for him or her and in his or her name, place or stead, in any and all capacities, to sign any and all amendments to this Registration Statement (including post-effective amendments), and to sign any registration statement for the same offering covered by this Registration Statement that is to be effective upon filing pursuant to Rule 462(b) promulgated under the Securities Act, and all post-effective amendments thereto, and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing requisite and necessary to be done in and about the premises, as fully to all intents and purposes as he or she might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact and agents, or their, his or her substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Act of 1933, as amended, this Registration Statement has been signed by the following persons in the capacities and on the dates indicated.
| Signature |
Title |
Date | ||
| /s/ Isaac E. Ciechanover Isaac E. Ciechanover, M.D. |
President, Chief Executive Officer and Director (principal executive officer) | June 29, 2015 | ||
| /s/ John F. McGrath, Jr. John F. McGrath, Jr. |
Chief Financial Officer (principal financial and accounting officer) | June 29, 2015 | ||
| /s/ Eric L. Dobmeier Eric L. Dobmeier |
Director | June 29, 2015 | ||
| /s/ Matthew K. Fust Matthew K. Fust |
Director | June 29, 2015 | ||
| /s/ Carol Gallagher Carol Gallagher, Pharm.D. |
Director | June 29, 2015 | ||
| /s/ Joel S. Marcus Joel S. Marcus |
Director | June 29, 2015 | ||
| /s/ Beth Seidenberg Beth Seidenberg, M.D. |
Director | June 29, 2015 | ||
| /s/ Eckard Weber Eckard Weber, M.D. |
Director | June 29, 2015 | ||
II-4
EXHIBIT INDEX
| Exhibit |
Incorporated by Reference | Filed | ||||||||||
| Exhibit Description |
Form | File No. | Exhibit | Filing Date | ||||||||
| 1.1* | Form of Underwriting Agreement | |||||||||||
| 3.1 | Amended and Restated Certificate of Incorporation of Atara Biotherapeutics, Inc. | S-1 | 333-196936 | 3.4 | 06/20/2014 | |||||||
| 3.2 | Amended and Restated Bylaws of Atara Biotherapeutics, Inc. | S-1 | 333-196936 | 3.4 | 06/20/2014 | |||||||
| 4.1 | Form of Common Stock Certificate | S-1/A | 333-196936 | 4.1 | 07/10/2014 | |||||||
| 4.2 | Investor Rights Agreement, by and among Atara Biotherapeutics, Inc. and the stockholders named therein, dated March 31, 2014 | S-1 | 333-196936 | 4.2 | 06/20/2014 | |||||||
| 5.1* | Opinion of Cooley LLP | |||||||||||
| 10.1 | 2014 Equity Incentive Plan | S-1/A | 333-196936 | 10.1 | 07/10/2014 | |||||||
| 10.2 | Forms of Option Agreement and Option Grant Notice under the 2014 Equity Incentive Plan | S-1 | 333-196936 | 10.2 | 06/20/2014 | |||||||
| 10.3 | Form of Restricted Stock Unit Agreement and Restricted Stock Unit Grant Notice under the 2014 Equity Incentive Plan | S-1 | 333-196936 | 10.3 | 06/20/2014 | |||||||
| 10.4 | Nina Biotherapeutics, Inc. 2012 Equity Incentive Plan | S-1 | 333-196936 | 10.4 | 06/20/2014 | |||||||
| 10.5 | Pinta Biotherapeutics, Inc. 2012 Equity Incentive Plan | S-1 | 333-196936 | 10.5 | 06/20/2014 | |||||||
| 10.6 | Santa Maria Biotherapeutics, Inc. 2012 Equity Incentive Plan | S-1 | 333-196936 | 10.6 | 06/20/2014 | |||||||
| 10.7 | Form of Stock Unit Agreement under the Nina Biotherapeutics, Inc. 2012 Equity Incentive Plan, Pinta Biotherapeutics, Inc. 2012 Equity Incentive Plan and Santa Maria Biotherapeutics, Inc. 2012 Equity Incentive Plan | S-1 | 333-196936 | 10.7 | 06/20/2014 | |||||||
| 10.8 | 2014 Employee Stock Purchase Plan | S-1/A | 333-196936 | 10.8 | 07/10/2014 | |||||||
| 10.9 | Form of Indemnification Agreement made by and between Atara Biotherapeutics, Inc. and each of its directors and executive officers | S-1 | 333-196936 | 10.9 | 06/20/2014 | |||||||
| 10.10 | Amended and restated offer letter agreement between Atara Biotherapeutics, Inc. and Isaac E. Ciechanover, dated March 31, 2014 | S-1 | 333-196936 | 10.10 | 06/20/2014 | |||||||
| Exhibit |
Incorporated by Reference | Filed | ||||||||||
| Exhibit Description |
Form | File No. | Exhibit | Filing Date | ||||||||
| 10.11 | Amended and restated offer letter agreement between Atara Biotherapeutics, Inc. and Christopher Haqq, dated March 31, 2014 | S-1 | 333-196936 | 10.11 | 06/20/2014 | |||||||
| 10.12 | Amended and restated offer letter agreement between Atara Biotherapeutics, Inc. and John F. McGrath, Jr., dated March 31, 2014 | S-1 | 333-196936 | 10.12 | 06/20/2014 | |||||||
| 10.13 | Amended and restated offer letter agreement between Atara Biotherapeutics, Inc. and Mitchall G. Clark, dated March 31, 2014 | S-1 | 333-196936 | 10.13 | 06/20/2014 | |||||||
| 10.14 | Amended and restated offer letter agreement between Atara Biotherapeutics, Inc. and Gad Soffer, dated March 31, 2014 | S-1 | 333-196936 | 10.14 | 06/20/2014 | |||||||
| 10.15† | Exclusive License Agreement, by and between Amgen Inc. and Nina Biotherapeutics, Inc., dated as of September 7, 2012 | S-1/A | 333-196936 | 10.15 | 07/10/2014 | |||||||
| 10.16† | Amendment No. 1 to Exclusive License Agreement, by and between Amgen Inc. and Nina Biotherapeutics, Inc., dated as of October 22, 2012 | S-1 | 333-196936 | 10.16 | 06/20/2014 | |||||||
| 10.17† | Amendment No. 2 to Exclusive License Agreement, by and between Amgen Inc. and Nina Biotherapeutics, Inc., dated as of September 7, 2012 | S-1 | 333-196936 | 10.17 | 06/20/2014 | |||||||
| 10.18† | Exclusive License Agreement, by and between Amgen Inc. and Pinta Biotherapeutics, Inc., dated as of September 7, 2012 | S-1/A | 333-196936 | 10.18 | 07/10/2014 | |||||||
| 10.19† | Amendment No. 1 to Exclusive License Agreement, by and between Amgen Inc. and Pinta Biotherapeutics, Inc., dated as of October 22, 2012 | S-1 | 333-196936 | 10.19 | 06/20/2014 | |||||||
| 10.20† | Amendment No. 2 to Exclusive License Agreement, by and between Amgen Inc. and Pinta Biotherapeutics, Inc., dated as of June 28, 2013 | S-1 | 333-196936 | 10.20 | 06/20/2014 | |||||||
| 10.21† | Exclusive License Agreement, by and between Amgen Inc. and Santa Maria Biotherapeutics, Inc., dated as of September 7, 2012 | S-1/A | 333-196936 | 10.21 | 07/10/2014 | |||||||
| Exhibit |
Incorporated by Reference | Filed | ||||||||||
| Exhibit Description |
Form | File No. | Exhibit | Filing Date | ||||||||
| 10.22† | Amendment No. 1 to Exclusive License Agreement, by and between Amgen Inc. and Santa Maria Biotherapeutics, Inc., dated as of October 22, 2012 | S-1 | 333-196936 | 10.22 | 06/20/2014 | |||||||
| 10.23† | Amendment No. 2 to Exclusive License Agreement, by and between Amgen Inc. and Santa Maria Biotherapeutics, Inc., dated as of July 29, 2013 | S-1 | 333-196936 | 10.23 | 06/20/2014 | |||||||
| 10.24† | Amendment No. 3 to Exclusive License Agreement, by and between Amgen Inc. and Santa Maria Biotherapeutics, Inc., dated as of April 4, 2014 | S-1 | 333-196936 | 10.24 | 06/20/2014 | |||||||
| 10.25 | Office Lease, by and between Atara Biotherapeutics, Inc. and Freeway Properties III, dated as of August 12, 2013 | S-1 | 333-196936 | 10.25 | 06/20/2014 | |||||||
| 10.26 | Sublease, by and between Atara Biotherapeutics, Inc. and XDX, Inc., dated as of January 10, 2013 | S-1 | 333-196936 | 10.26 | 06/20/2014 | |||||||
| 10.27 | Consent to Sublease, by and among Atara Biotherapeutics, Inc., XDX, Inc. and BMR-Bayshore Boulevard LLC, dated as of January 14, 2013 | S-1 | 333-196936 | 10.27 | 06/20/2014 | |||||||
| 10.28 | Sublease Agreement, by and between Atara Biotherapeutics, Inc. and Accesia, Inc., dated as of September 11, 2014 | S-1/A | 333-196936 | 10.28 | 09/26/2014 | |||||||
| 10.29† | Exclusive Option Agreement, by and between Atara Biotherapeutics, Inc. and Memorial Sloan Kettering Cancer Center, dated as of September 19, 2014 | 10-Q | 001-36548 | 10.29 | 05/11/2015 | |||||||
| 10.30** | Exclusive License Agreement, by and between Atara Biotherapeutics, Inc. and Memorial Sloan Kettering Cancer Center, dated as of June 12, 2015 | X | ||||||||||
| 21.1 | List of subsidiaries. | 10-K/A | 001-36548 | 21.1 | 03/06/2015 | |||||||
| 23.1 | Consent of Independent Registered Public Accounting Firm | X | ||||||||||
| 23.2* | Consent of Cooley LLP (see Exhibit 5.1) | |||||||||||
| 24.1 | Power of Attorney (see page II-4) | X | ||||||||||
| * | To be filed by amendment |
| † | Confidential treatment has been granted for a portion of this exhibit. |
| ** | The registrant has requested confidential treatment for a portion of this exhibit. |